Regional anesthesia is a valuable diagnostic aid used to localize lameness when, after a thorough clinical examination, the site of pain remains uncertain. Localizing pain allows other diagnostic procedures, such as anesthesia of a joint, radiography, ultrasonography, CT, scintigraphy, or MRI to be used more effectively and economically to identify the cause of lameness. Additionally, use of regional anesthesia allows some surgical procedures to be performed without the need for general anesthesia, and it can be used to provide temporary, humane relief of pain.
Lidocaine HCl (2%) and mepivacaine HCl (2%) are the local anesthetic agents most commonly used to induce regional anesthesia during the lameness examination. Mepivacaine HCl is preferred by most clinicians, because it causes less tissue reaction than lidocaine HCl. Bupivacaine HCl is used to induce regional anesthesia for humane relief of pain, because it provides anesthesia that lasts 4–6 hr.

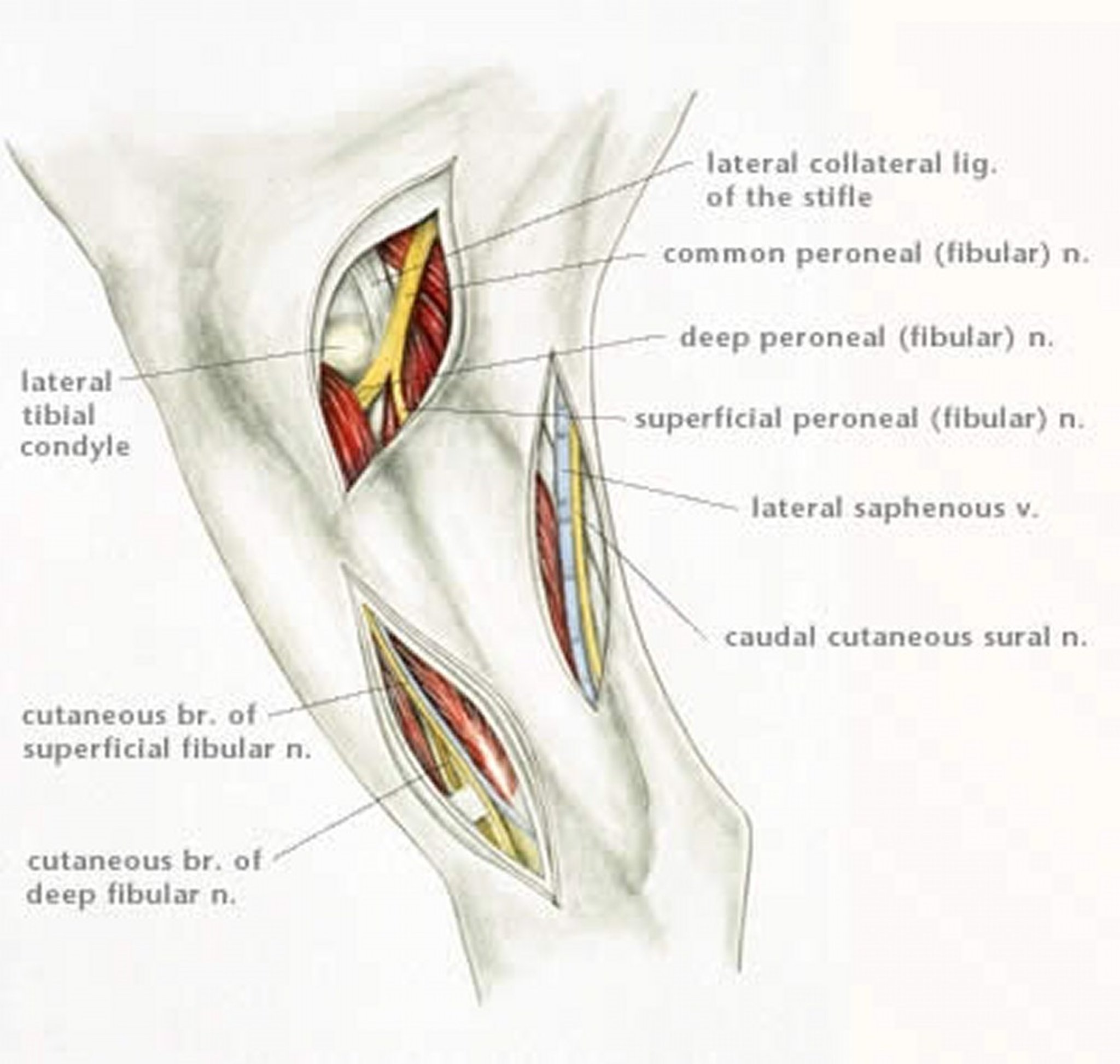
Illustration by Dr. Gheorghe Constantinescu.

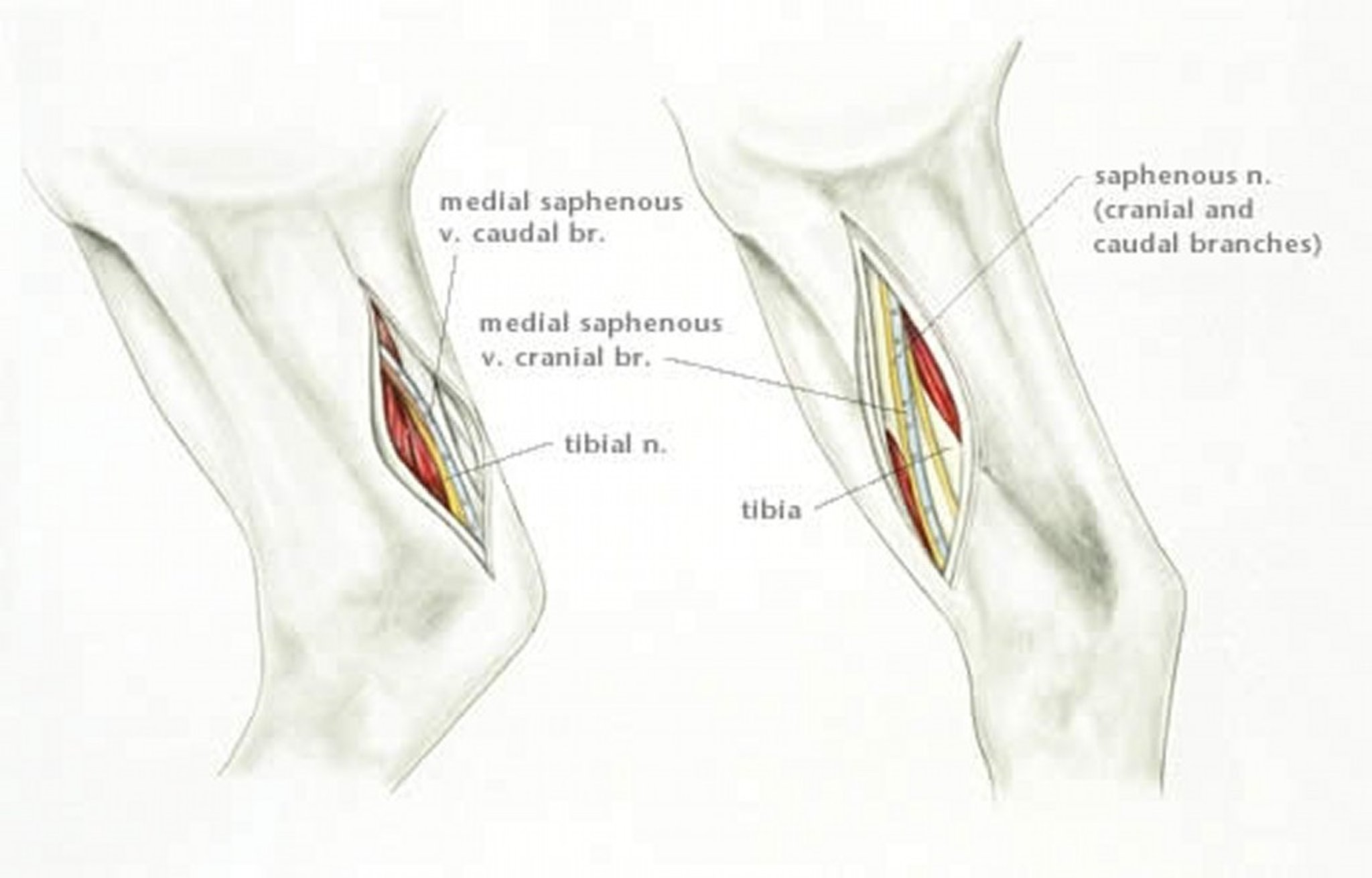
Illustration by Dr. Gheorghe Constantinescu.

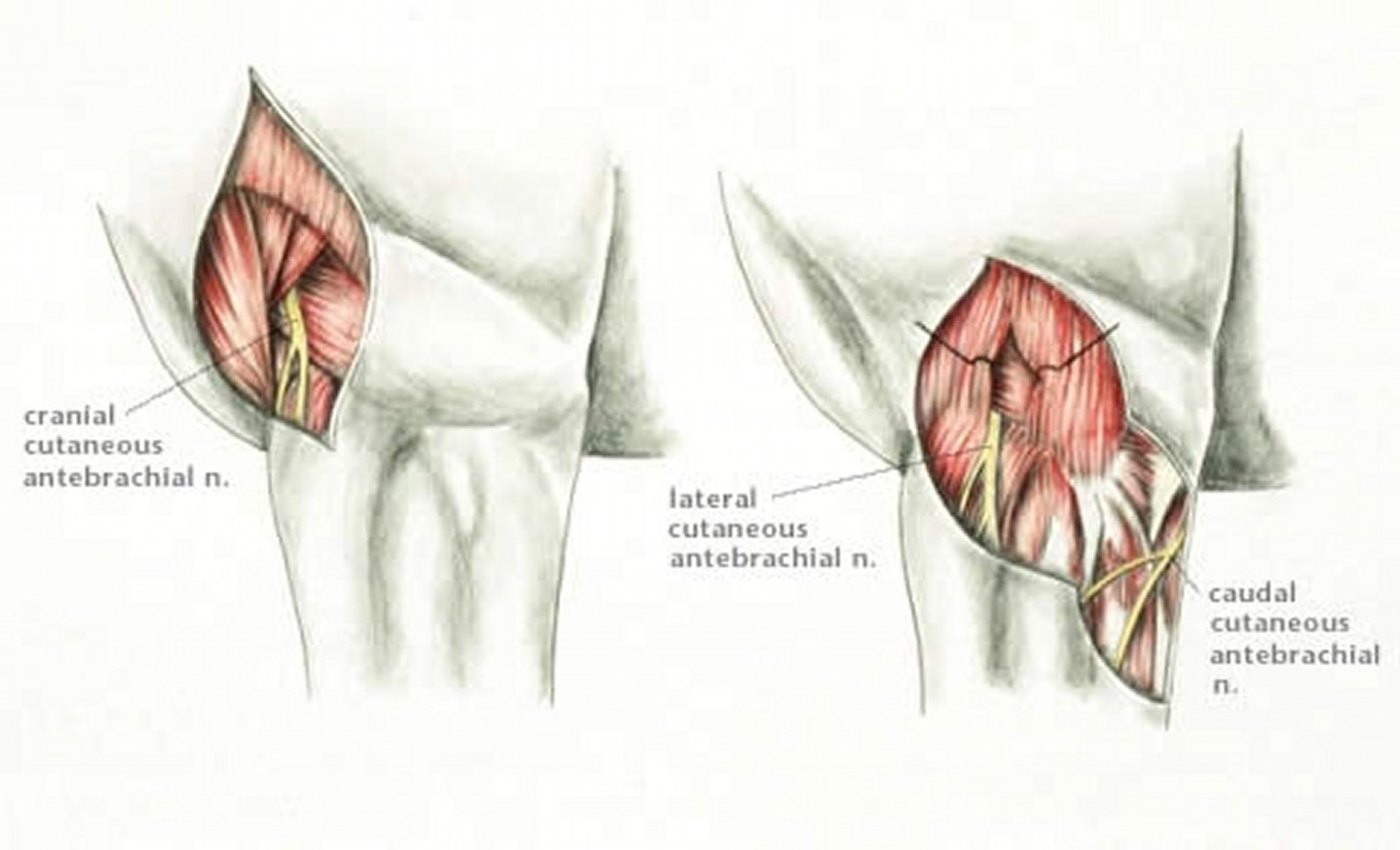
Illustration by Dr. Gheorghe Constantinescu.

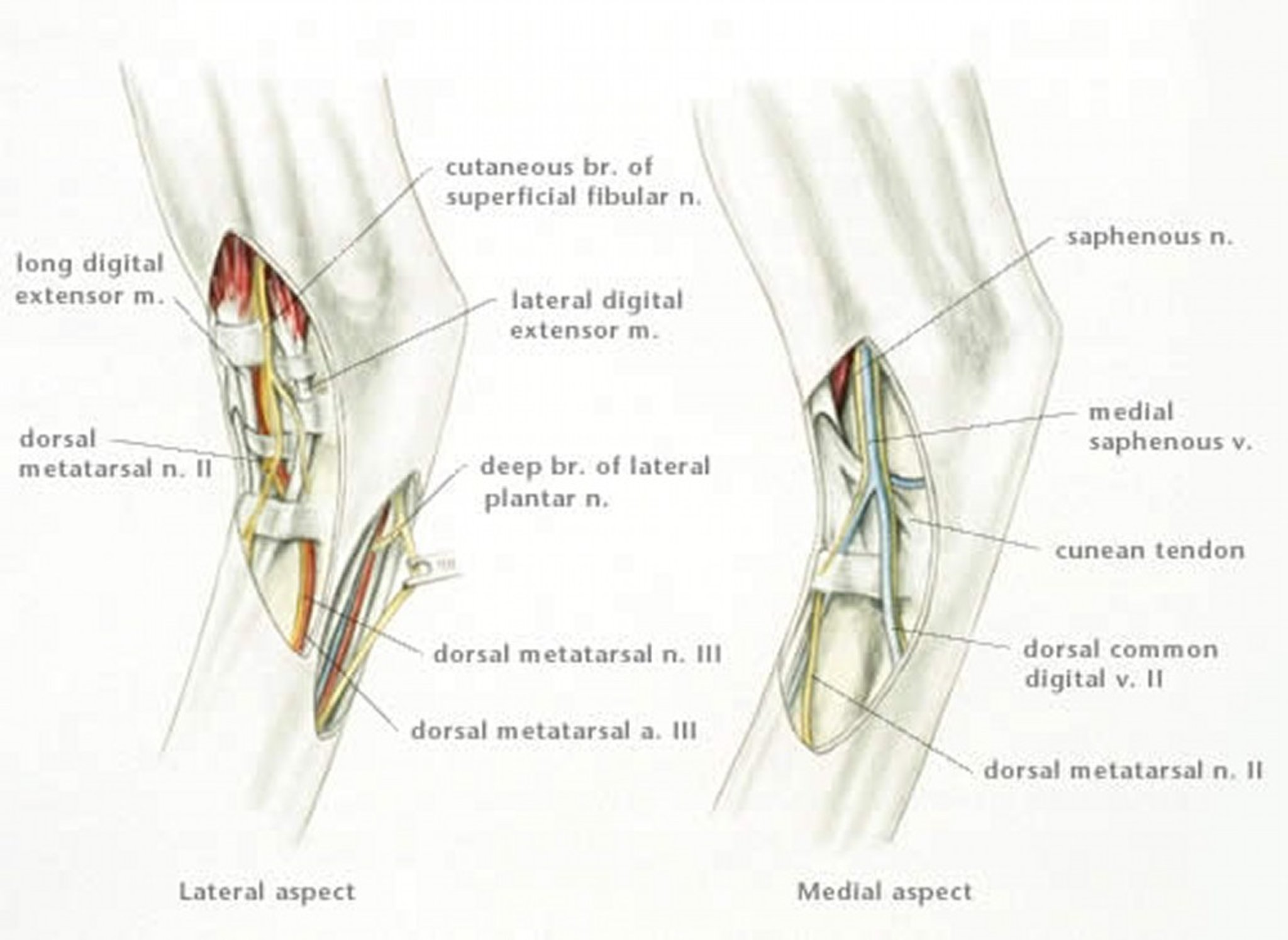
Illustration by Dr. Gheorghe Constantinescu.

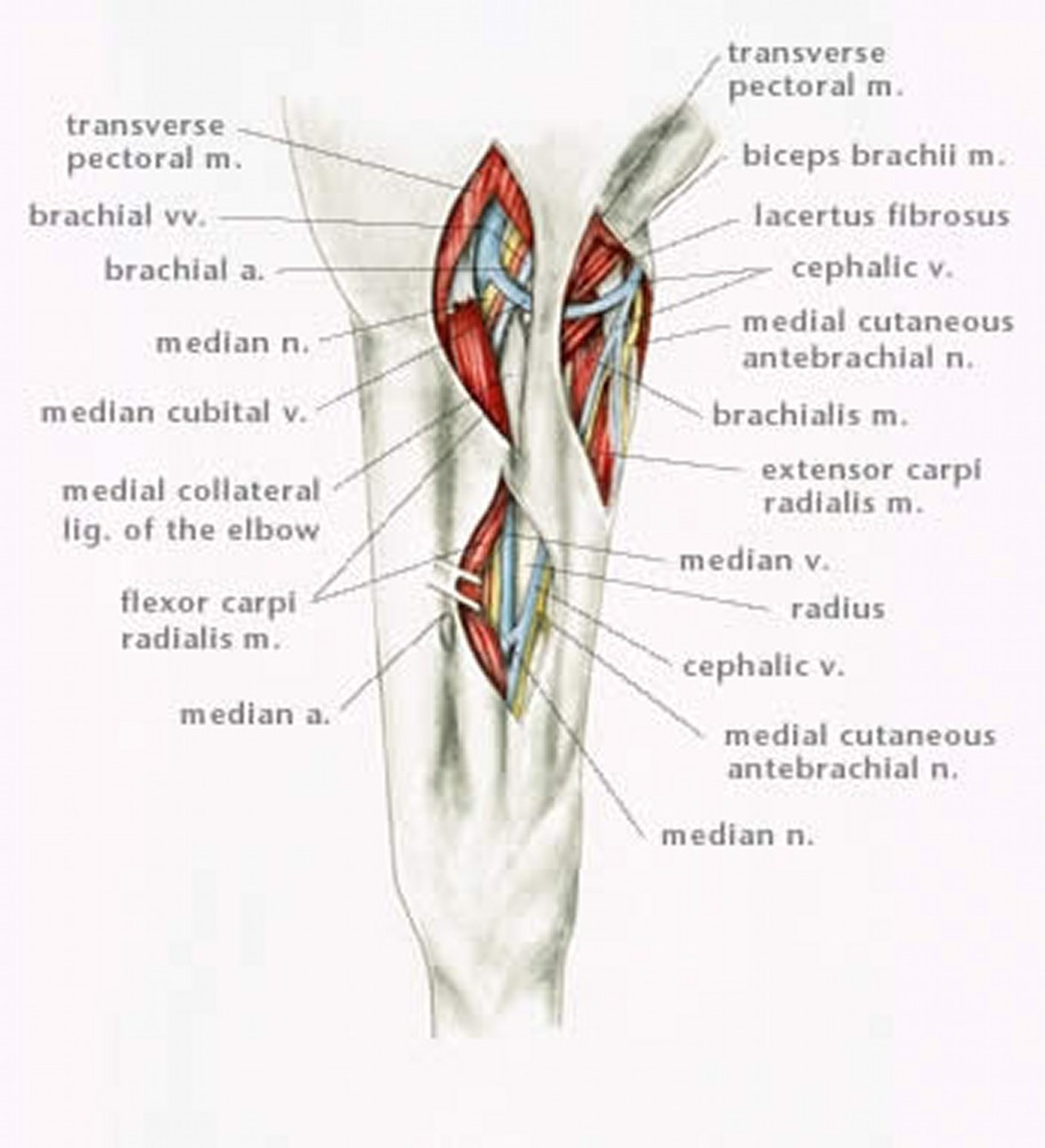
Illustration by Dr. Gheorghe Constantinescu.
The choice of anesthetic agent may depend on its duration of action. The anesthetic effect of mepivacaine HCl, which lasts 90–120 min, makes this agent valuable for examining a horse with lameness in multiple limbs or if multiple sites of pain on a limb are suspected. Lidocaine HCl, which has an anesthetic effect of only 30–45 min, might be the preferred local anesthetic agent when different techniques of diagnostic analgesia are likely to be used during the lameness examination.
Most nerves below the carpus or hock are anesthetized using a 25-gauge, 5/8-in. (1.59-cm) needle. A 1½-in. (3.8-cm), larger-gauge needle (eg, 22- or 20-gauge) is used to anesthetize nerves located more proximally on the limb. If a relatively large-gauge needle is to be used, SC deposition of a small amount of local anesthetic solution, using a 25-gauge needle, may avoid resentment by the horse when the larger-gauge needle is inserted.
To avoid broken or bent needles during perineural administration of local anesthetic solution, the needle should always be inserted detached from the syringe. Spinal needles are flexible and more likely to bend than break and, thus, safer to use if there is a possibility the horse may move the limb. Using a flexible needle is especially important when the difference in range of movement between skin and deeper tissues is large, in case the horse moves during injection. Luer-lock syringes should not be used because they are difficult to attach to the needle after it is inserted, and this type of syringe cannot be detached quickly from the needle to prevent the needle from being pulled out, bent, or broken if the horse moves during the procedure. The needle should be directed distally during insertion when anesthetizing nerves in the distal portion of the limb. Directing the needle proximally may result in proximal migration of anesthetic solution and unintended anesthesia of more proximal branches of the nerve, thus confusing the results of the examination.
When the goal of regional anesthesia is to identify a site of pain below the carpus or hock, only the smallest effective volume of anesthetic solution should be administered to avoid inadvertent anesthesia of adjacent nerves. When the nerve can be palpated subcutaneously, a very small volume of local analgesic solution can be used because the solution can be placed more accurately into the fascia surrounding the nerve.
Before regional anesthesia is performed, the horse should be consistently and sufficiently lame so that any improvement in gait can be detected. Lungeing or riding the horse may exacerbate a subtle lameness. The lameness of some horses improves or resolves during exercise; for these horses, a false-positive response to regional anesthesia may result if the horse has not been sufficiently exercised before it is examined. If a horse is subtly lame, using a wireless, inertial sensor–based system designed to evaluate lameness allows objective interpretation of results of diagnostic analgesia.
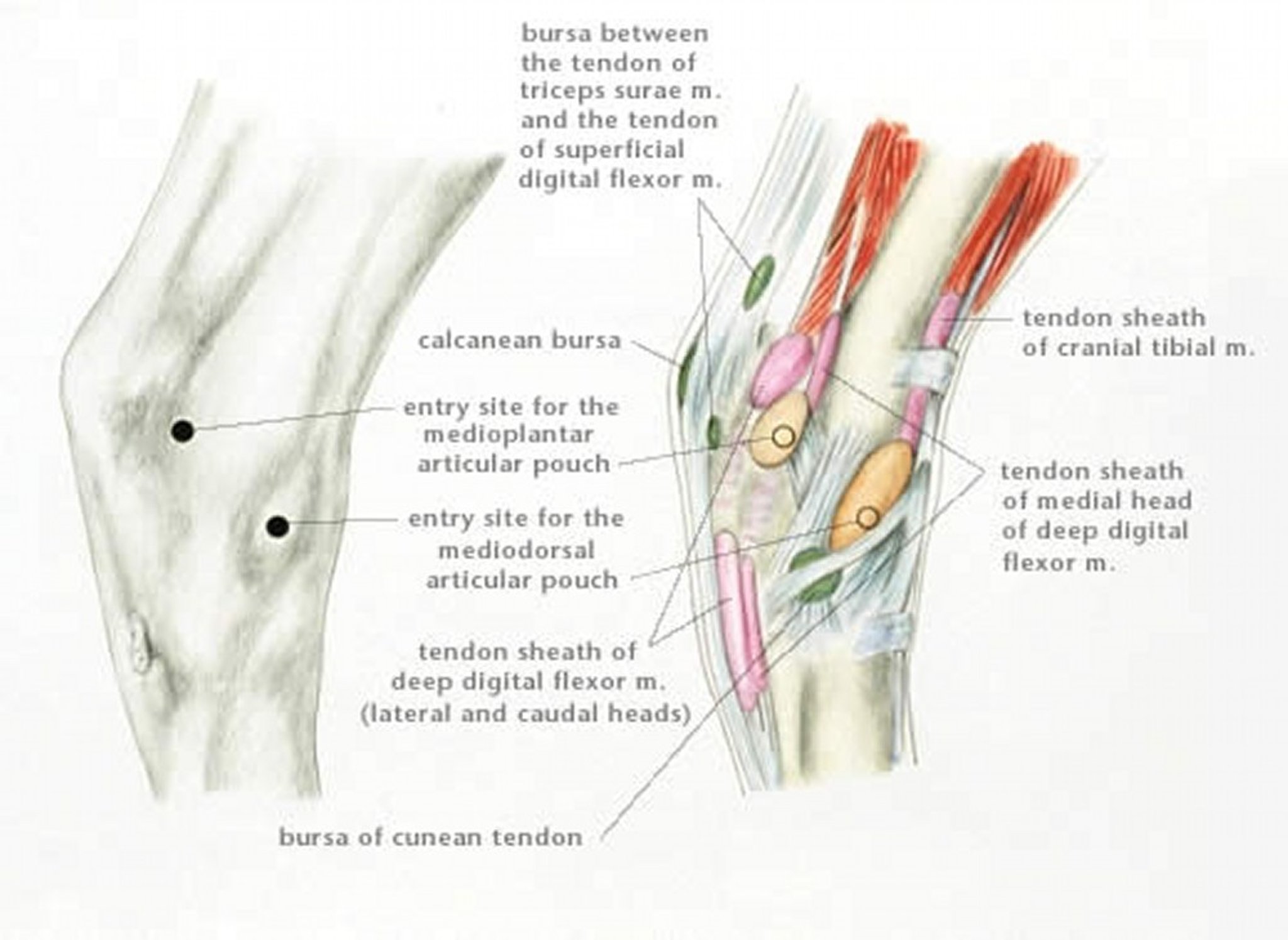
Illustration by Dr. Gheorghe Constantinescu.

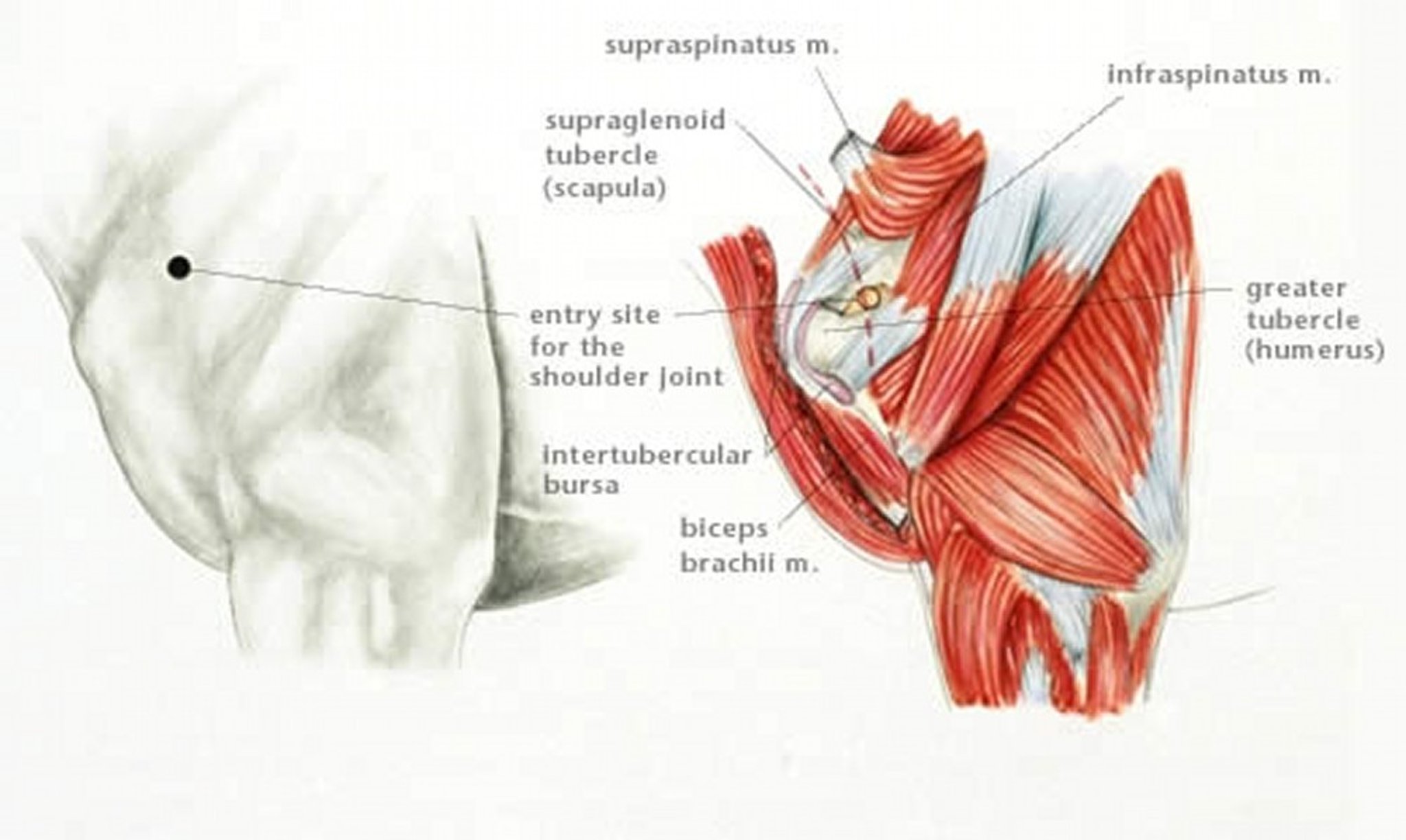
Illustration by Dr. Gheorghe Constantinescu.

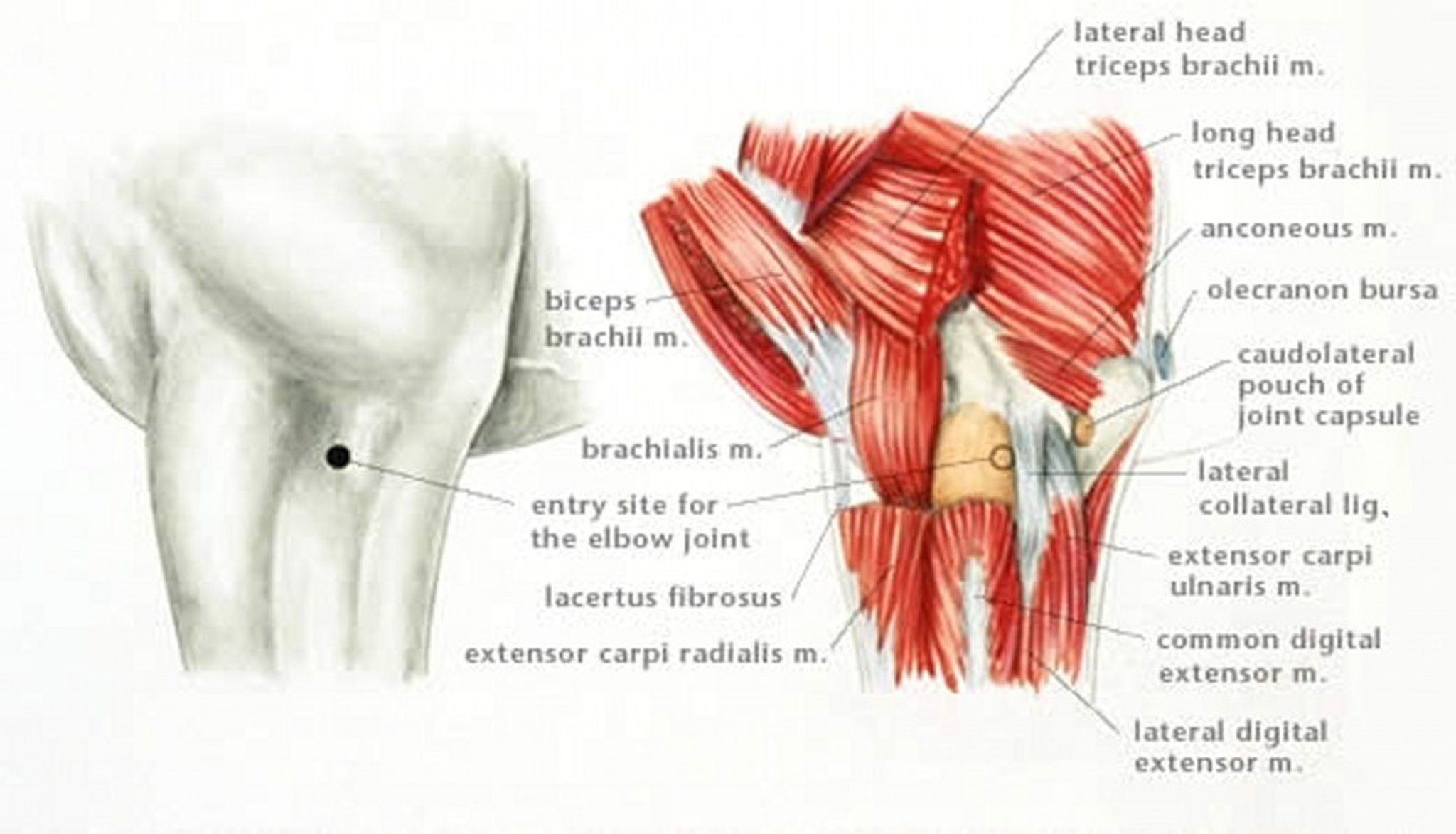
Illustration by Dr. Gheorghe Constantinescu.

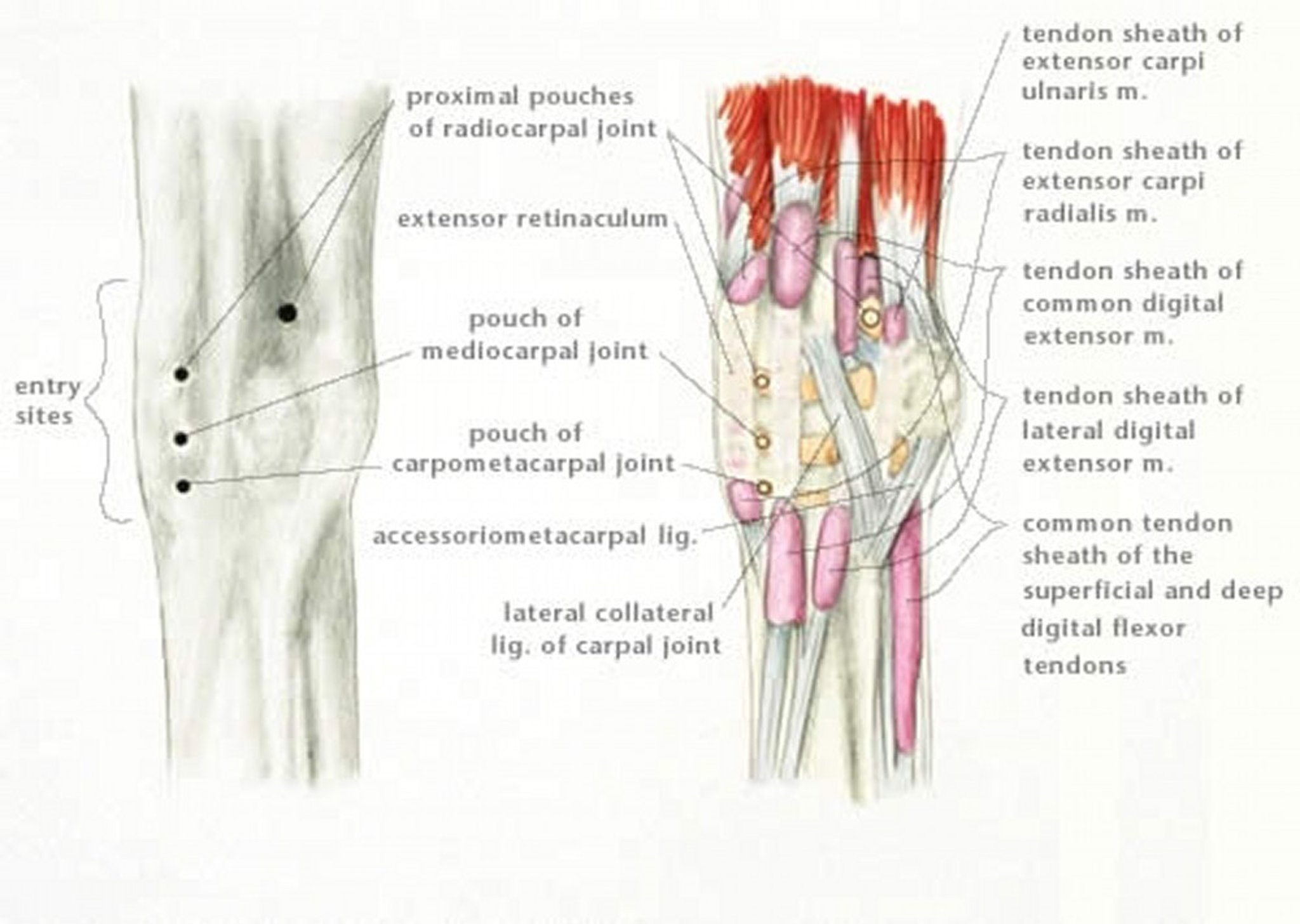
Illustration by Dr. Gheorghe Constantinescu.
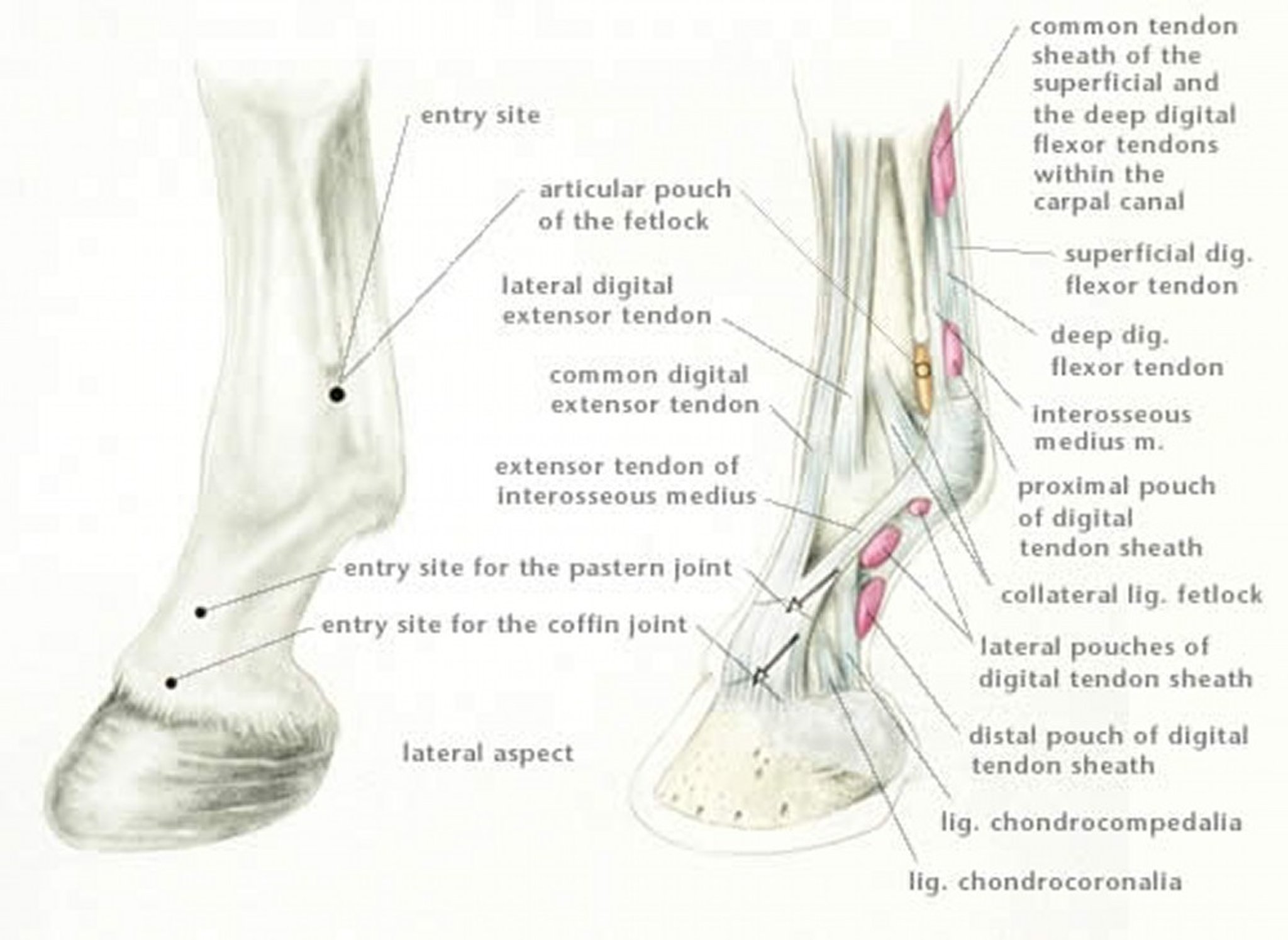
Illustration by Dr. Gheorghe Constantinescu.

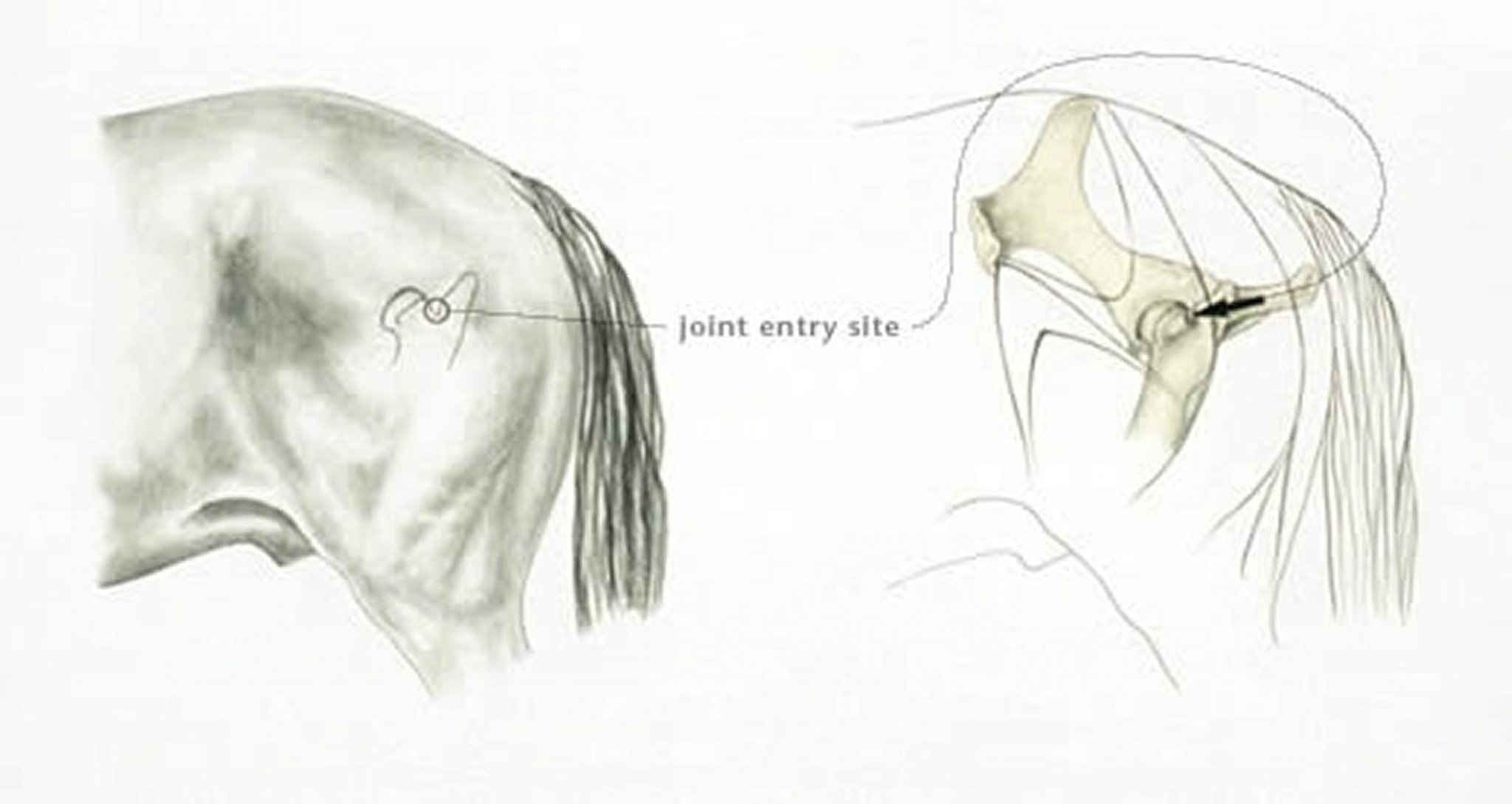
Illustration by Dr. Gheorghe Constantinescu.
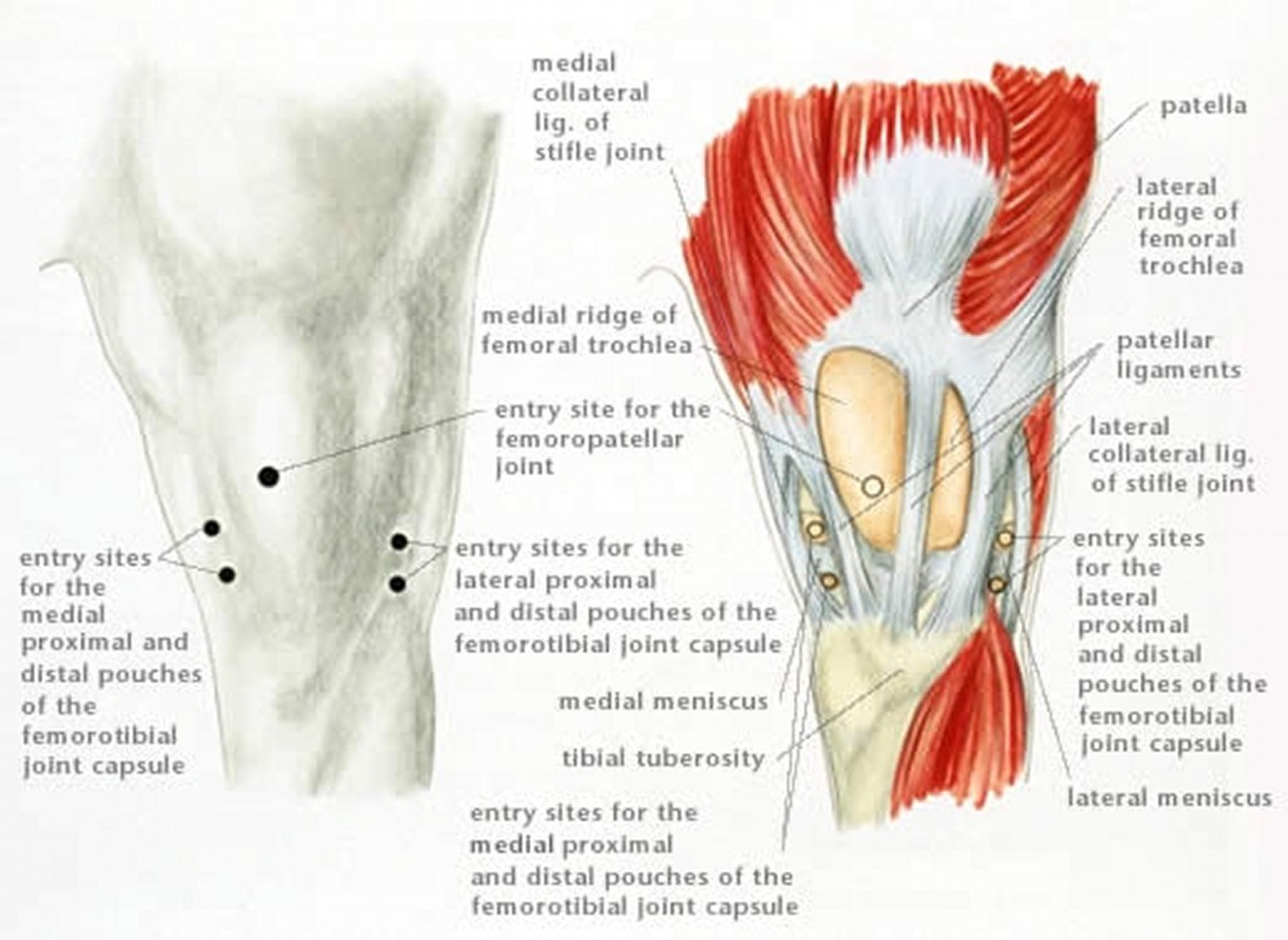
Illustration by Dr. Gheorghe Constantinescu.
Relief of pain and resolution of lameness after local anesthetic solution is administered into the fascia surrounding a nerve in the distal portion of the limb usually occurs within 5 min, but anesthesia of larger nerves in the proximal portion of the limb may take 20–40 min. Results of a regional nerve block can be misinterpreted if the horse’s gait is assessed before the onset of pain relief. When assessing the effects of anesthesia of nerves in the distal portion of the limb, the clinician should keep in mind that anesthetic solution might migrate up the nerve to anesthetize more proximal structures, thus confusing the results of the examination. To avoid this complication, the gait should be evaluated within 15 min after administering a regional nerve bock in the distal portion of the limb. When a regional nerve block is administered in the proximal portion of the limb, the horse may develop a gait abnormality or stumble because of altered proprioception. When nerves above the hock or carpus are anesthetized, it may be prudent to assess the horse’s gait on a soft surface or after bandaging the distal portion of the limb so that abrasion to skin over the dorsum of the fetlock is avoided if the horse stumbles.
If the gait is unchanged after regional anesthesia, the effectiveness of the nerve block should be determined by checking for skin sensation within the dermatome expected to be desensitized. Skin sensation is assessed by pressing the tip of a ballpoint pen, key, or similar instrument over the skin covering the region intended to be desensitized. For a fractious horse, skin sensation is more safely checked with the limb held or from a distance using a blunt instrument taped to a 3-ft pole. A well-behaved, stoic horse may not react to stimulation of skin even though regional anesthesia was ineffective. For such a horse, reaction to cutaneous stimulation should be assessed before regional anesthesia is performed, or reaction to cutaneous stimulation of the same dermatome on the contralateral limb should be assessed.
When performing regional anesthesia, especially in the distal portion of the limb, local anesthetic solution can be administered inadvertently into a blood vessel, joint, tendon sheath, or bursa. Aspiration before injection may indicate that the needle has been placed within a blood vessel. Administering the anesthetic solution as the needle is withdrawn decreases the likelihood of depositing the solution in an unintended structure and results in deposition of the solution in more than one tissue plane, which increases the likelihood of the solution contacting the nerve.
Opinions vary concerning the amount of skin preparation necessary before administering regional anesthesia. For short-haired horses, the site of injection is often prepared by wiping the site with cotton pledgets or gauze sponges soaked in 70% isopropyl alcohol until a pledget or sponge appears clean. If the site of injection is particularly dirty, it should be scrubbed with antiseptic soap. The consequences of a nonsterile, SC injection are usually minimal, but inadvertent, nonsterile injection of a tendon sheath or joint could result in septic synovitis.
Regional anesthesia of the distal portion of the limb can be accomplished in most horses using minimal restraint, but for fractious horses or for horses previously subjected to regional anesthesia, using a lip twitch or lip chain is prudent. The twitch works best when applied immediately before placing the needle. If this does not provide sufficient restraint, xylazine (0.2 mg/kg) or detomidine (10 mcg/kg) can be given IV. Acepromazine has no analgesic effect and, therefore, is less likely to ameliorate lameness than is a sedative, such as xylazine or detomidine, which provides some analgesia. In fact, some clinicians claim that acepromazine accentuates subtle lameness, possibly by making the horse less aware of its environment and, therefore, more aware of pain in the lame limb. The degree to which sedation or tranquilization interferes with assessment of gait depends on the severity of lameness and the skill of the clinician performing the examination.
Restraining the horse in stocks to administer regional anesthesia of the distal portion of the limb increases the likelihood of injury to the clinician. Regional anesthesia of the distal portion of the limb usually requires multiple injections, which is most safely accomplished with the limb held. When a nerve block is performed with the horse’s limb on the ground, the contralateral limb can be lifted off the ground to enhance the safety of the procedure for the clinician.
When anesthetizing the foot of a forelimb, most clinicians prefer to hold the limb while facing in the opposite direction as the horse; however, some clinicians prefer to anesthetize the foot while facing the same direction as the horse. When facing the same direction as the horse, the foot can be held between the clinician’s knees to free both hands for the procedure, but the clinician is at risk of injury if the horse swings its limb caudally. When the clinician faces the opposite direction as the horse, the procedure is performed using one hand because the other hand must hold the limb.
Nerve blocks performed distal to the fetlock of the pelvic limb are most safely performed with the pelvic limb stretched caudally and held on the thigh of the clinician performing the block.
Complications of regional nerve blocks are rare but include a broken needle shaft, SC infection, and infection of a synovial structure adjacent to the nerve anesthetized. Local anesthetic solution is detectable systemically, which could create a problem for a horse participating in a competition if the horse’s serum is examined for the presence of drugs.
Regional Anesthesia of the Forelimb
Because perineural analgesia should start distally and progress proximally, the palmar digital nerve (PDN) block is the most commonly performed regional nerve block of the forelimb. The PDN block is performed with the limb held. The needle is inserted directly over the palpable neurovascular bundle ~1 cm proximal to the cartilage of the foot. The needle is directed distally, and 1.5 mL of local anesthetic solution is deposited near the junction of the nerve and the cartilage of the foot. The PDN block is sometimes called a “heel block,” but this terminology is erroneous because the block anesthetizes the entire foot, including the distal interphalangeal (coffin) joint. For a few horses, the PDN block may also cause at least partial anesthesia of the proximal interphalangeal (pastern) joint, especially if a large volume of local anesthetic solution (eg, >3 mL) is injected.
If the horse’s gait does not improve after a PDN block, some clinicians next administer a semi-ring block at the pastern to anesthetize the dorsal branches of the digital nerve that supply the foot. Because the dorsal branches of the digital nerve contribute little to sensation within the foot, a semi-ring block at the pastern is unlikely to improve the gait if a PDN block failed to improve it.
Most clinicians proceed to a basisesamoid nerve block if the horse’s lameness is not reduced with a PDN block. With this regional nerve block, the palmar nerves are anesthetized at the level of the base of the proximal sesamoid bones, before the nerve branches into the dorsal and palmar digital nerves. When performing an abaxial sesamoid nerve block, 2.5–3 mL of local anesthetic solution is deposited at the base of the proximal sesamoid bones over the neurovascular bundle, which is easily palpated at this location. More proximal deposition of local anesthetic solution may anesthetize a portion of the fetlock joint. Positive response to a basisesamoid nerve block, performed after a PDN block has failed to ameliorate lameness, localizes the site of pain causing lameness to the pastern.
The low palmar nerve block, or low 4-point block, is performed after a negative response to the abaxial sesamoid nerve block. This nerve block is usually performed with the horse bearing weight on the limb, but it can also be performed with the limb held. The medial and lateral palmar nerves are anesthetized, using a 25-gauge, 5/8-in. needle, by depositing 2 mL of local anesthetic solution over each palmar nerve where it lies subcutaneously at the dorsal border of the deep digital flexor tendon. The palmar nerves should be blocked at the level of the metacarpus to avoid the possibility of misdirecting a needle into the digital flexor sheath, which often extends proximally to the level of the end of the splint bones. When the palmar nerves are blocked at the level of the middle of the metacarpus, the communicating branch that connects them, the ramus communicans, should also be blocked with 1 mL of local anesthetic solution. Blocking one palmar nerve proximal to the ramus communicans and the other distal to it allows sensory impulses to propagate through the ramus from the side blocked proximal to the ramus and then proximally through the palmar nerve blocked distal to the ramus. Though easily palpated on the forelimb, the ramus communicans is often nonexistent or impossible to palpate on the pelvic limb. To complete the 4-point block, 1–2 mL of local anesthetic solution is deposited SC at the distal end of each splint bone, where the palmar metacarpal nerve lies next to the periosteum of the third metacarpal bone. A positive response to a low 4-point block, performed after a negative response to an abaxial sesamoid nerve block, localizes the site of pain causing lameness to the fetlock.
The high palmar nerve block, or high 4-point block, can be performed when the low 4-point block fails to improve lameness. With the limb bearing weight, the medial and lateral palmar and palmar metacarpal nerves are anesthetized slightly distal to the level of the carpometacarpal joint. To anesthetize a palmar nerve, a 25-gauge, 5/8-in. needle is inserted through fascia to where the nerve lies near the dorsal border of the deep digital flexor tendon, and 3–5 mL of anesthetic solution is deposited over the nerve.
Anesthetizing the medial and lateral palmar nerves alone desensitizes the flexor tendons and inferior check ligament. With the limb held or bearing weight, the palmar metacarpal nerves are anesthetized slightly distal to the level of the carpometacarpal joint by inserting a 20- to 22-gauge, 1 ½-in. needle into the angle formed by the junction of the third metacarpal bone and the second or fourth metacarpal bone. Anesthetizing the medial and lateral palmar metacarpal nerves alone desensitizes the splint bones and their interosseous ligaments and the proximal aspect of the suspensory ligament.
An easier alternative to the high palmar nerve block, when the site of pain causing lameness is suspected to be in the proximal portion of suspensory ligament, is the lateral palmar nerve block, which is performed, with the limb bearing weight, by inserting a 25-gauge, 5/8-in. needle over the lateral palmar nerve where it courses over the medial aspect of the accessory carpal bone. The needle is inserted in a medial to lateral direction at the distal third of a palpable groove, and 2 mL of local anesthetic solution is deposited. Because the medial and lateral palmar metacarpal nerves arise from the deep branch of the lateral palmar nerve distal to this site, the structures they innervate, such as the proximal aspect of the suspensory ligament, are desensitized.

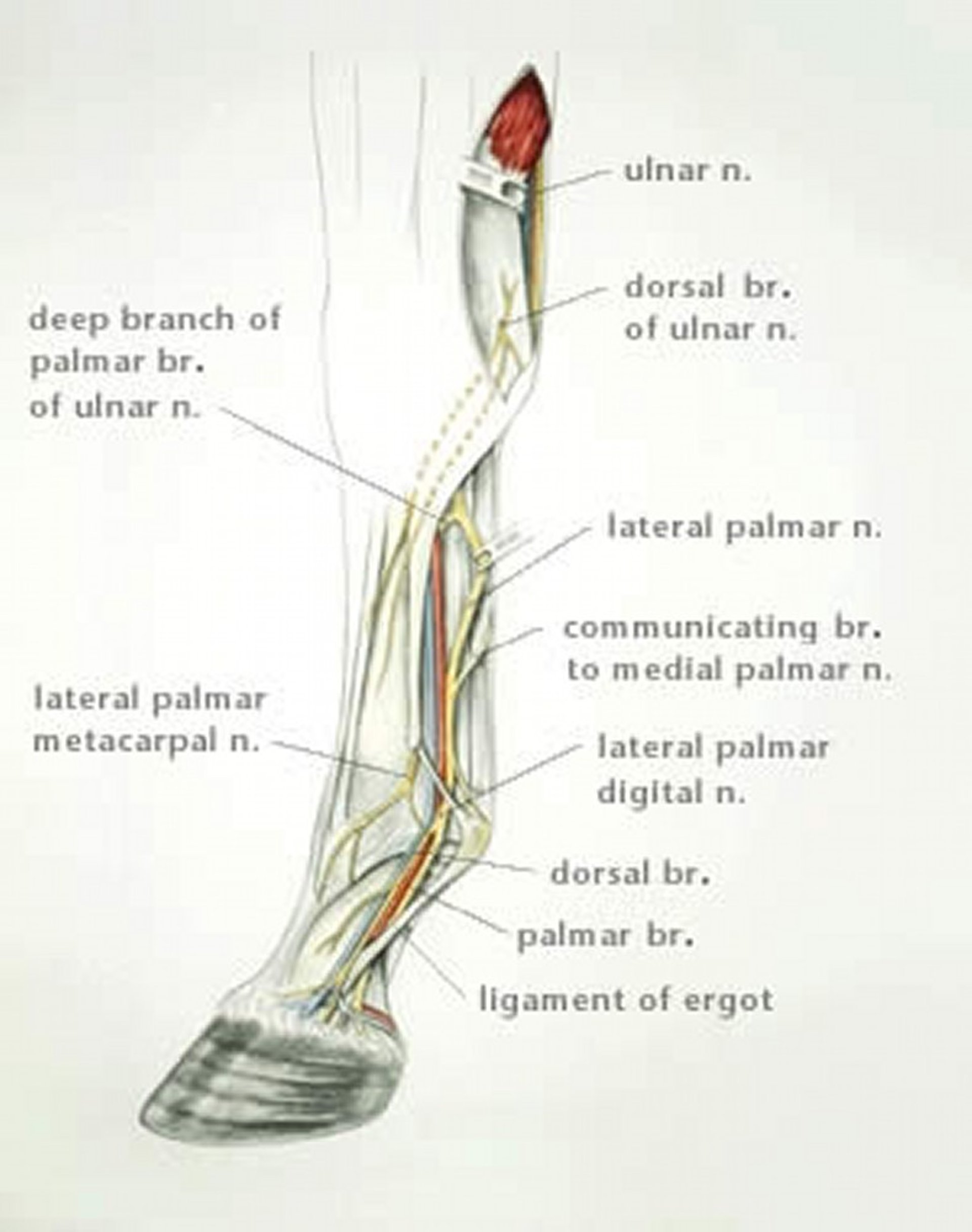
Illustration by Dr. Gheorghe Constantinescu.

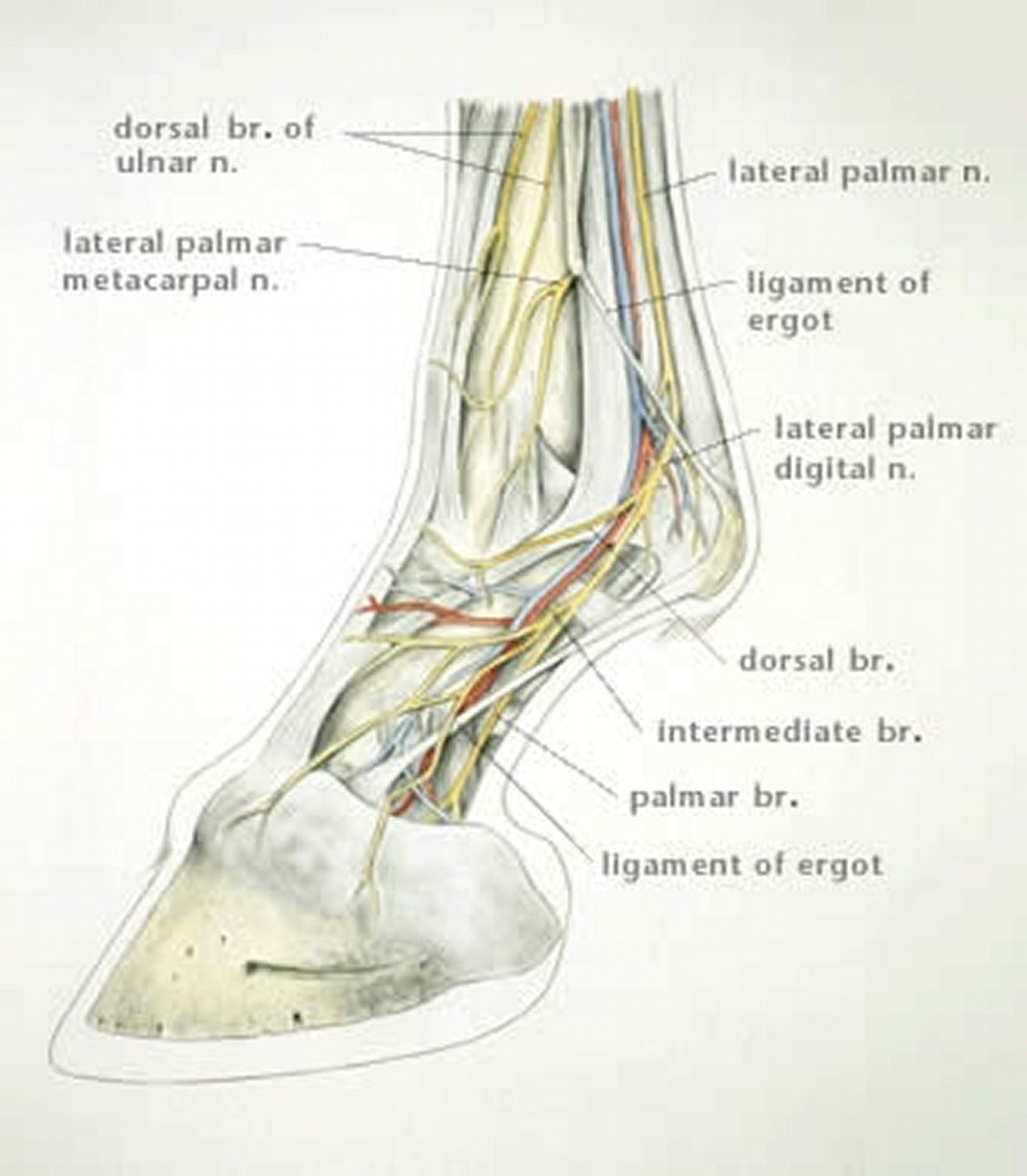
Illustration by Dr. Gheorghe Constantinescu.
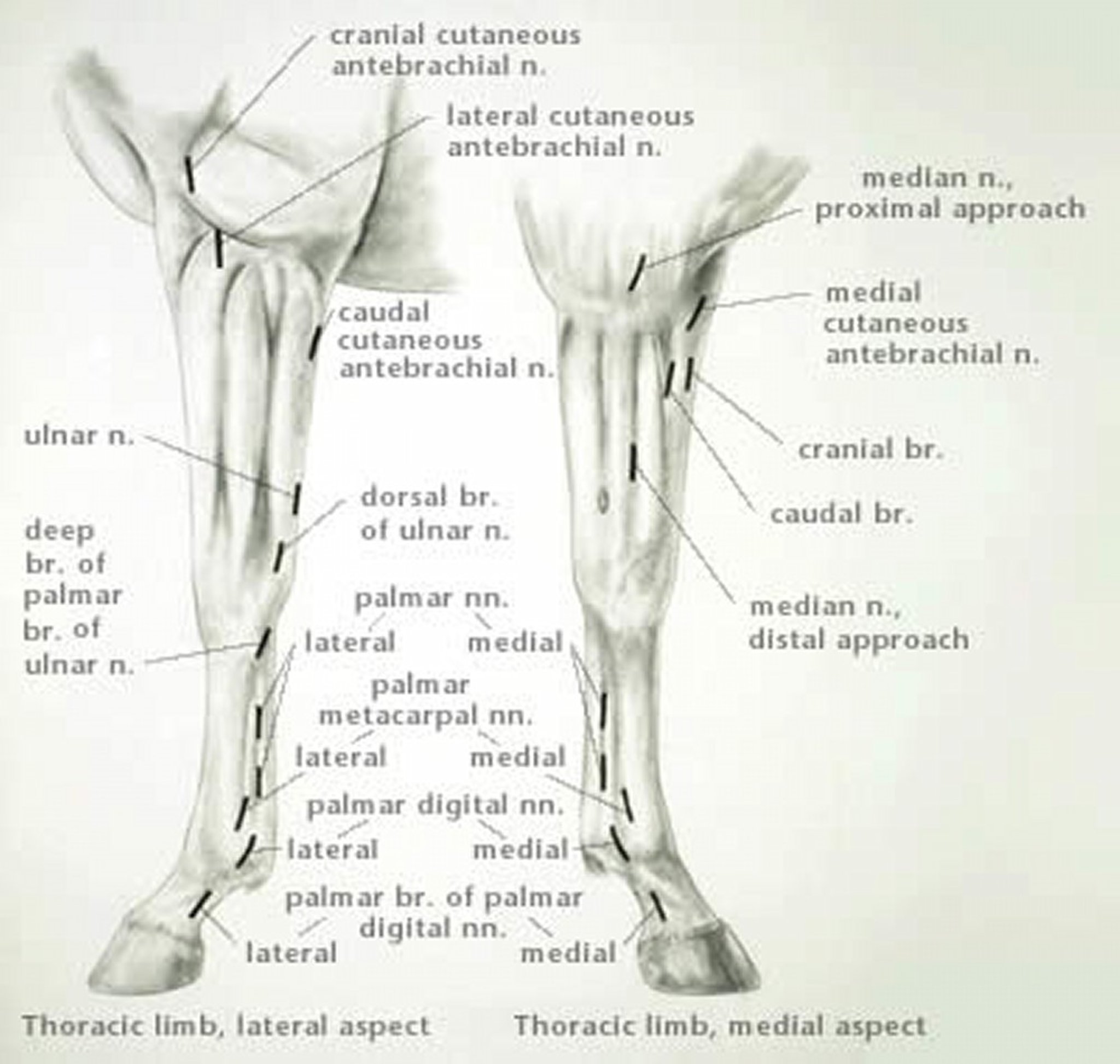
Illustration by Dr. Gheorghe Constantinescu.
If the site of pain causing lameness cannot be localized by performing the previously discussed nerve blocks, most clinicians perform joint blocks of the carpus, elbow, or shoulder. The order in which these synovial structures are desensitized is not important. The median and ulnar nerves are sometimes anesthetized simultaneously as part of a lameness evaluation to exclude pain below the elbow as the cause of lameness, but more commonly, they are anesthetized along with the medial cutaneous antebracheal nerve to allow surgery of the limb without the need for general anesthesia.
Regional Anesthesia of the Pelvic Limb
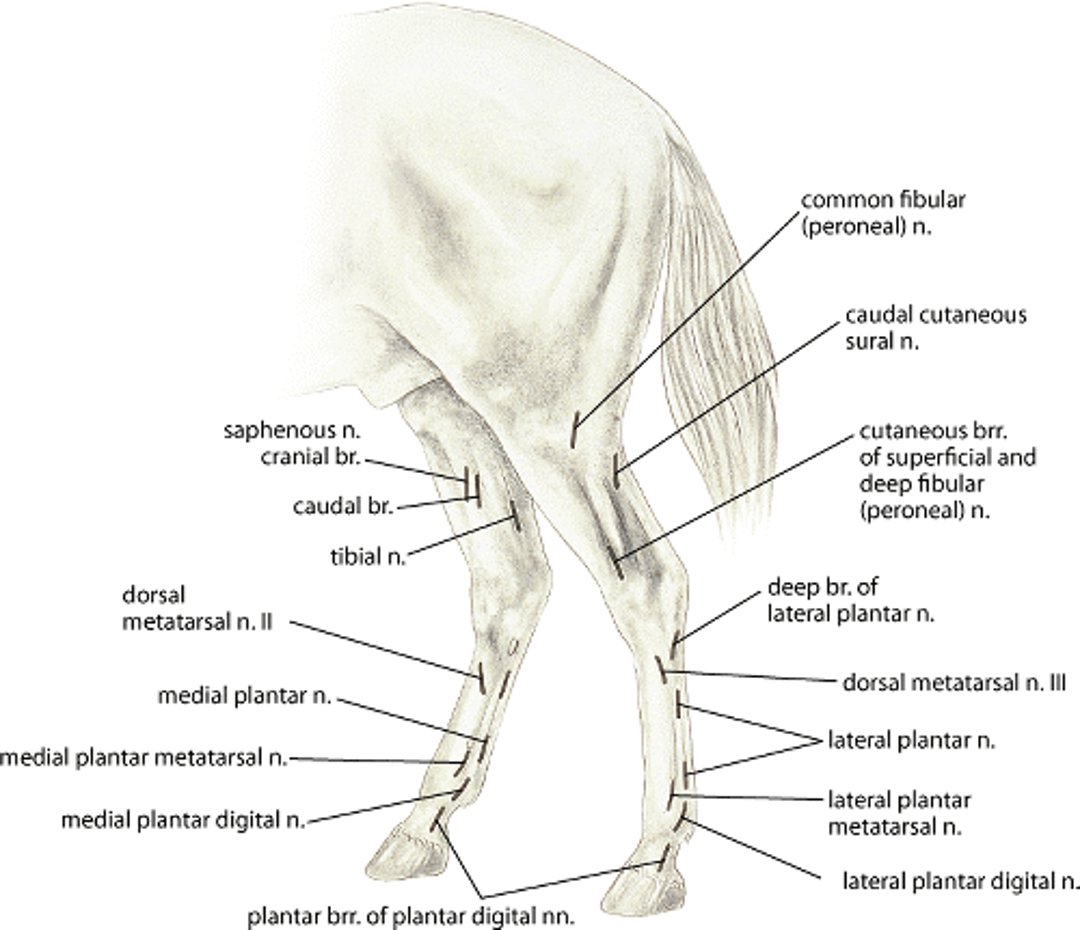
Techniques to administer regional anesthesia of the distal portion of the pelvic limb are slightly different than the techniques to administer regional anesthesia of the forelimb, because branches of the deep peroneal (fibular) nerve of the pelvic limb supply additional innervation to this region. These branches, the medial and lateral dorsal metatarsal nerves, course adjacent to the extensor tendon and innervate the dorsal aspect of the laminar corium. After depositing local anesthetic solution for a low 4-point nerve block at the level of the distal aspect of the splint bones, the needle is redirected dorsolaterally or dorsomedially, parallel to the bearing surface of the foot, and an additional 2 mL of local anesthetic solution is deposited SC to anesthetize the medial or lateral dorsal metatarsal nerves. Most lamenesses of the pelvic limb, however, can be evaluated accurately without anesthetizing the dorsal metatarsal nerves.
The high plantar nerve block is administered, using techniques similar to those used to administer the high palmar nerve block, ~1 cm distal to the tarsometatarsal joint. When the proximal aspect of the suspensory ligament is suspected to be the site of pain causing lameness, 3–4 mL of local anesthetic solution can be deposited through a 20- to 23-gauge, 1-in. needle, axial to the lateral splint bone and ~1 cm distal to the tarsometatarsal joint, between the tendon of the deep digital flexor muscle and the suspensory ligament. The solution diffuses to anesthetize the deep branch of the lateral plantar nerve, which branches into the medial and lateral plantar metatarsal nerves that supply the proximal aspect of the suspensory ligament.
Depending on results of flexion tests or causes of lameness typical for the particular athletic function of the horse, the clinician may proceed to joint blocks or to more proximal regional nerve blocks. The peroneal and tibial nerves can be blocked simultaneously to exclude pain in the hock or regions distal to the hock as a cause of lameness, or the blocks can be performed separately to gain added insight as to the possible site of pain. If lameness is ameliorated after a tibial nerve block, but not after a low 4- or 6- point block, the suspensory ligament is a likely source of pain. If lameness is ameliorated after a peroneal (fibular) nerve block, but not after a low 4- or 6- point block, one or more of the tarsal joints are the likely source of pain.
The tibial nerve is blocked ~10 cm above the point of the hock on the medial aspect of the limb, where it lies in fascia on caudal surface of the deep flexor muscle, cranial to the Achilles tendon. Twenty mL of mepivacaine HCl is deposited through a 20-gauge, 1½- in. (3.8-cm) needle at this site, in at least several planes in the fascia surrounding the nerve. The deep peroneal nerve can be blocked on the lateral aspect of the limb ~4 in. above the point of the hock in the groove formed by the lateral and long digital extensor muscles. A 20-gauge, 1½-in. needle is directed slightly caudally until it contacts the caudal edge of the tibia, and 20 mL of mepivacaine HCl is deposited.
Landmarks for nerve block of the horse pelvic limb
Landmarks for nerve block of the horse pelvic limb. Illustration by Dr. Gheorghe Constantinescu. |