




Corneal foreign bodies are frequently observed in domestic animals. They are usually organic material; however, sand, metal, and glass foreign bodies are also observed (see superficial corneal foreign body image).
Clinical signs associated with corneal foreign bodies include variable blepharospasm, tearing, and a variable reflex uveitis (aqueous flare, miosis, iridal swelling, ocular hypotony, and possible hypopyon).

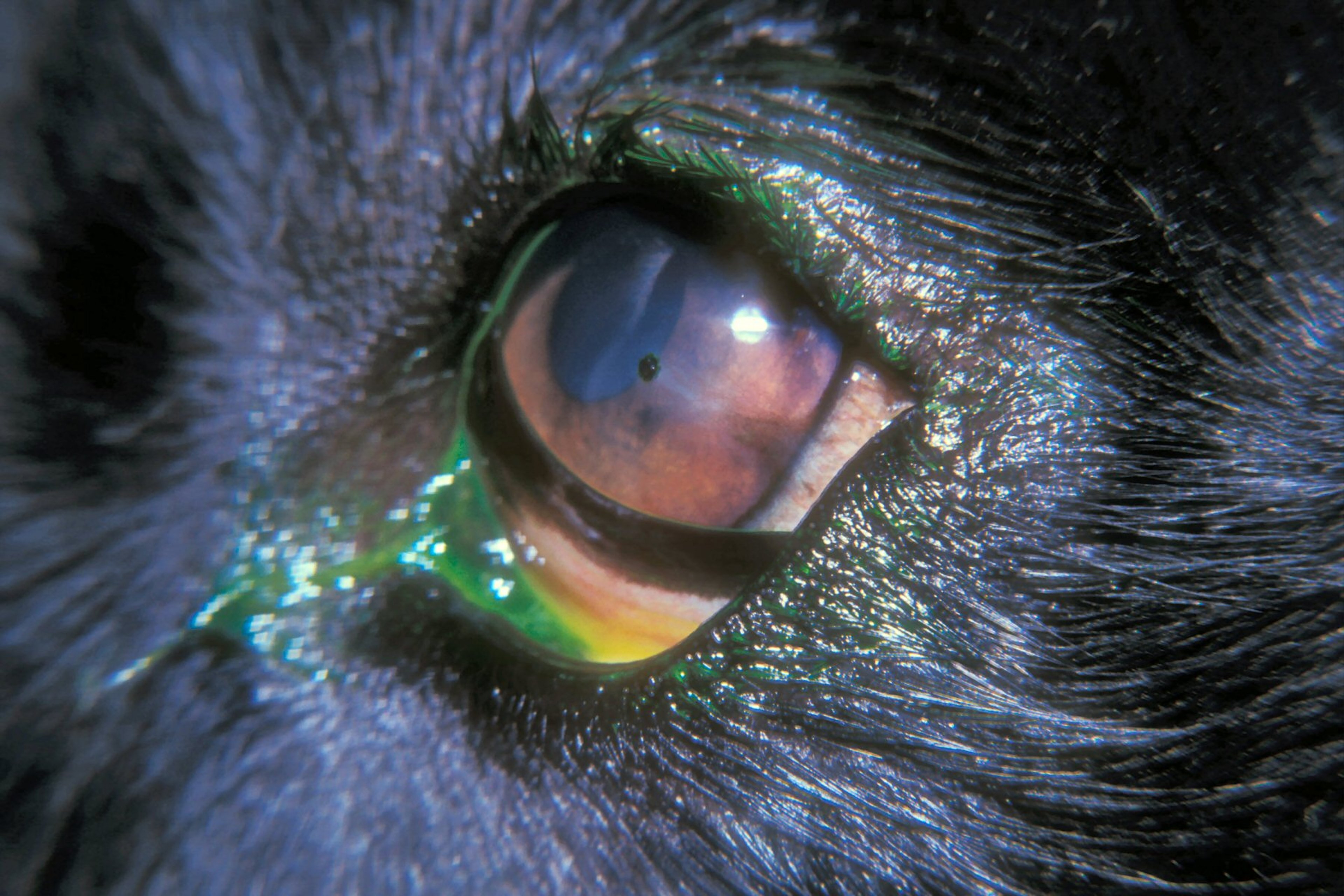
Courtesy of Dr. K. Gelatt.
Foreign bodies can be identified on the conjunctival surface, in the posterior third eyelid fornix, or on or in the cornea. Those that adhere to the ocular surfaces are usually removed under topical anesthesia with either vigorous irrigation or small, serrated ophthalmic forceps.
If the foreign body has embedded within the deeper corneal layers or has penetrated into the anterior chamber, general anesthesia is required for careful removal from either the anterior corneal surface or the anterior chamber.
It is imperative that the location of the foreign body (ie, depth within the cornea) be established before its removal. If in doubt, it should be assumed that it penetrates into the anterior chamber.
The corneal wound is apposed with simple interrupted 7-0 to 9-0 absorbable sutures. Postoperative treatment typically includes topical and systemic broad-spectrum antimicrobials, mydriatics, and systemic NSAIDs.
Prognosis for vision is usually good. Infrequent complications include variable corneal scar formation, septic endophthalmitis, cataract formation, and secondary glaucoma.
For More Information
Belknap EB. Corneal emergencies. Top Companion Anim Med. 2015;30(3):74-80.
Also see pet health content regarding corneal injuries and foreign objects in the eye.







