

Anaplasmosis is a tickborne disease of ruminants caused by intracellular bacteria that infect red blood cells, causing fever and anemia. Diagnosis relies upon Giemsa-stained blood smears and serologic tests such as ELISA. Key treatments include tetracyclines and imidocarb; in some countries, less pathogenic species are used as live vaccines for the control of bovine anaplasmosis.
Anaplasmosis traditionally refers to a disease of ruminants caused by obligate intraerythrocytic bacteria of the order Rickettsiales, family Anaplasmataceae, genus Anaplasma. Cattle, sheep, goats, buffalo, and some wild ruminants can be infected with the erythrocytic Anaplasma. Anaplasmosis occurs in tropical and subtropical regions worldwide (~40°N to 32°S), including South and Central America, the USA, southern Europe, Africa, Asia, and Australia.
The Anaplasma genus also includes A phagocytophilum (compiled from species previously known as Ehrlichia phagocytophila, E equi, and human granulocytic ehrlichiosis agent, A bovis (formerly E bovis), and A platys (formerly E platys), all of which invade blood cells other than erythrocytes of their respective mammalian hosts. Bovine anaplasmosis is of economic significance in the cattle industry. A phagocytophilum is the causative agent of equine granulocytic ehrlichiosis.
Etiology and Pathogenesis of Anaplasmosis
Clinical bovine anaplasmosis is usually caused by A marginale. A centrale was isolated in South Africa from cattle with a mild disease and is often used as a vaccine to protect from A marginale infections. A ovis may cause mild to severe disease in sheep, deer, and goats and is less common than A marginale infection. A phagocytophilum has recently been reported to infect cattle; however, natural infection is rare and it does not cause clinical disease.
Transmission and Epidemiology of Anaplasmosis in Ruminants
Up to 17 different tick vector species (including Dermacentor, Rhipicephalus, Ixodes, Hyalomma, and Argas) have been reported to transmit Anaplasma spp (except A centrale found naturally in South Africa from R simus ticks only). Not all of these are likely significant vectors in the field, and it has been shown that strains of A marginale also coevolve with particular tick strains. Rhipicephalus (Boophilus) spp are major vectors of A marginale in Australia and Africa, and Dermacentor spp are the main vectors in the USA. Mechanical transmission via biting dipterans occurs in some regions. Anaplasmosis may also be spread through the use of contaminated needles or dehorning or other surgical instruments.
There is a strong correlation between age of cattle and severity of disease. Calves are much more resistant to disease (although not infection) than older cattle. This resistance is not due to colostral antibody from immune dams. In endemic areas where cattle first become infected with A marginale early in life, losses due to anaplasmosis are minimal. After recovery from the acute phase of infection, cattle remain chronically infected carriers but are generally immune to further clinical disease. However, these chronically infected cattle may relapse to anaplasmosis when immunosuppressed (eg, by corticosteroids), when infected with other pathogens, or after splenectomy. Carriers serve as a reservoir for further transmission. Serious losses occur when mature cattle with no previous exposure are moved into endemic areas or under endemically unstable situations when transmission rates are insufficient to ensure that all cattle are infected before reaching the more susceptible adult age.
Clinical Findings of Anaplasmosis
In animals < 1 year old, anaplasmosis is usually subclinical, in yearlings and 2-year-olds it is moderately severe, and in older cattle it is severe and often fatal. Anaplasmosis is characterized by progressive anemia due to extravascular destruction of infected and uninfected erythrocytes. The prepatent period of A marginale is directly related to the infective dose and typically ranges from 15–36 days (although it may be as long as 100 days). After the prepatent period, peracute (most severe but rare), acute, or chronic anaplasmosis may follow. Rickettsemia approximately doubles every 24 hours during the exponential growth phase. Generally, 10%–30% of erythrocytes are infected at peak rickettsemia, although this figure may be as high as 65%. RBC count, PCV, and hemoglobin values are all severely reduced. Macrocytic anemia with circulating reticulocytes may be present late in the disease.
Animals with peracute infections succumb within a few hours of the onset of clinical signs. Acutely infected animals lose condition rapidly. Milk production falls. Inappetence, loss of coordination, breathlessness when exerted, and a rapid, bounding pulse are usually evident in the late stages. The urine may be brown, but, in contrast to babesiosis, hemoglobinuria does not occur. A transient febrile response, with the body temperature rarely exceeding 106°F (41°C) occurs at about the time of peak rickettsemia. Mucous membranes appear pale and then yellow. Pregnant cows may abort. Surviving cattle convalesce over several weeks, during which hematologic parameters gradually return to normal.
Bos indicus breeds of cattle appear to possess a greater resistance to A marginale infection than B taurus breeds, but variation of resistance of individuals within breeds of both species occurs. Differences in virulence between Anaplasma strains and the level and duration of the rickettsemia also play a role in severity of clinical manifestations.
Lesions
Lesions are typical of those found in animals with anemia due to erythrophagocytosis. The carcasses of cattle that die from anaplasmosis are generally markedly anemic and jaundiced. Blood is thin and watery. The spleen is characteristically enlarged and soft, with prominent follicles. The liver may be mottled and yellow-orange. The gallbladder is often distended and contains thick brown or green bile. Hepatic and mediastinal lymph nodes appear brown. There are serous effusions in body cavities, pulmonary edema, petechial hemorrhages in the epi- and endocardium, and often evidence of severe GI stasis. Widespread phagocytosis of erythrocytes is evident on microscopic examination of the reticuloendothelial organs. A significant proportion of erythrocytes are usually found to be parasitized after death due to acute infection.
Diagnosis of Anaplasmosis
Diagnosis based on clinical signs, blood smears, and serologic testing

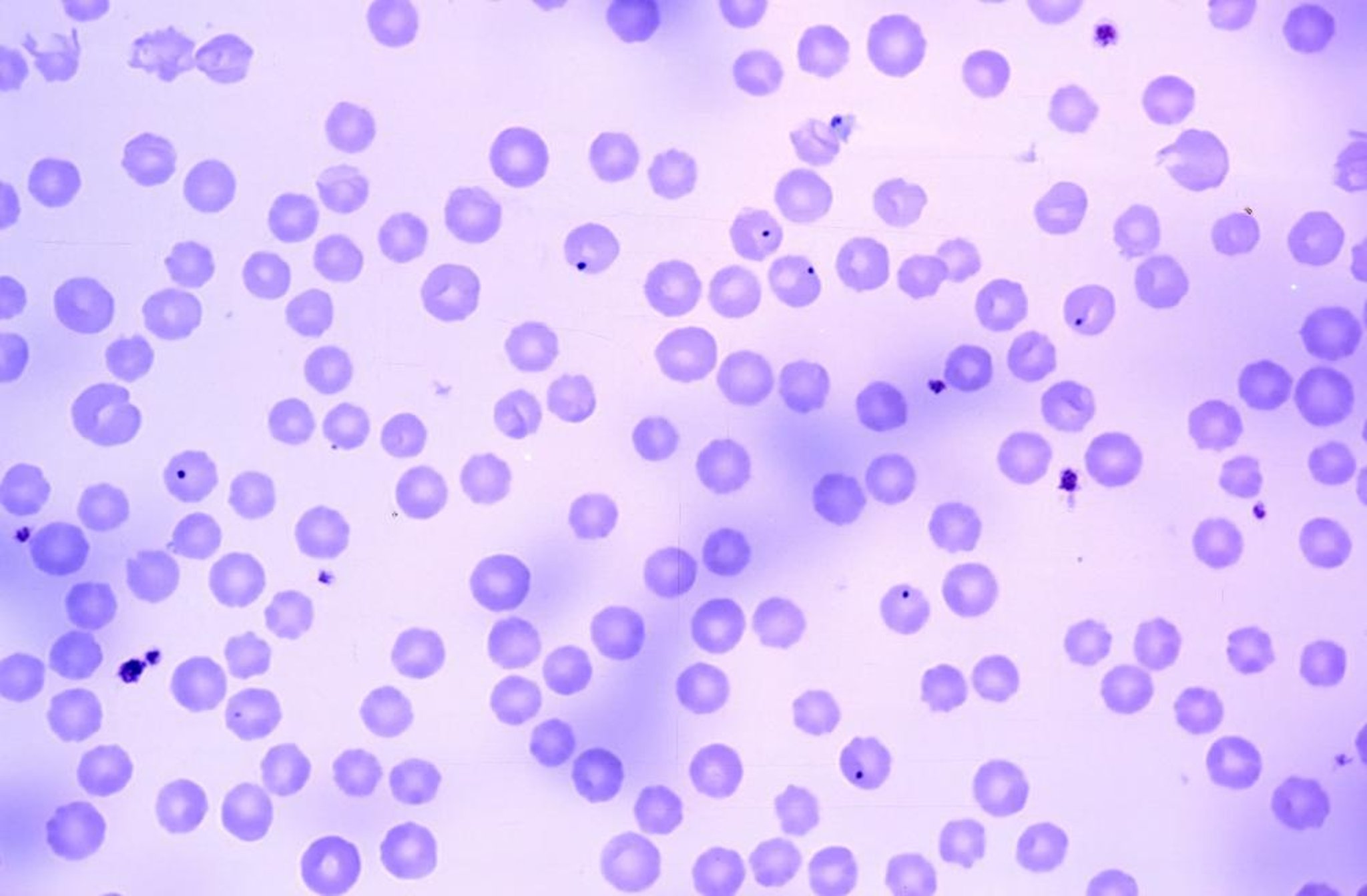
Anaplasma marginale in bovine blood, Wright-Giemsa, 100X oil immersion. Intracellular organisms appear as basophilic, spherical inclusions generally located near the margin of erythrocytes. Echinocytes are frequently present.
Courtesy of Ms. Sue Anderson, Tick Fever Centre, Wacol, Queensland, Australia.
A marginale, together with the hemoprotozoa Babesia bovis and B bigemina, are the causative agents of tick fever in cattle. These three species have similar geographic distributions, except that anaplasmosis occurs in the absence of babesiosis in the USA. Microscopic examination of Giemsa-stained thin and thick blood films is critical to distinguish anaplasmosis from babesiosis and other conditions that result in anemia and jaundice, such as leptospirosis and theileriosis. Blood in anticoagulant should also be obtained for hematologic testing. In Giemsa-stained thin blood films, Anaplasma spp appear as dense, homogeneously staining blue-purple inclusions 0.3–1 mcm in diameter. A marginale inclusions are usually located toward the margin of the infected erythrocyte, whereas A centrale inclusion bodies are located more centrally.
Inclusion bodies contain 1–8 initial bodies 0.3–0.4 mcm in diameter, which are the individual rickettsiae. The percentage of infected erythrocytes varies with the stage and severity of disease; maximum rickettsemias in excess of 50% can occur with A marginale. Microscopically, the infection becomes visible 2–6 weeks after transmission. During the course of infection, the rickettsemia can double each day for up to 10 days and then decreases. Severe anemia can persist for weeks after parasites cannot be detected in blood smears.
Chronically infected carriers may be identified with a fair degree of accuracy by serologic testing using the msp5 ELISA, complement fixation, or card agglutination tests. Nucleic acid-based detection methods are not always useful because these tests may not detect carrier levels.
At necropsy, thin blood films of liver, kidney, spleen, lungs, and peripheral blood should be prepared for microscopic examination.
Treatment, Control, and Prevention of Anaplasmosis
Tetracyclines, imidocarb, and vaccination by inoculation with less pathogenic species
Tetracycline antibiotics and imidocarb are currently used for treatment. Infections may be completely cleared by treatment with these drugs and the cattle then remain immune to severe anaplasmosis for at least 8 months.
Prompt administration of tetracycline drugs (tetracycline, chlortetracycline, oxytetracycline, rolitetracycline, doxycycline, minocycline) in the early stages of acute disease (eg, PCV >15%) usually ensures survival. A commonly used treatment consists of a single IM injection of long-acting oxytetracycline at a dosage of 20 mg/kg. Blood transfusion to partially restore the PCV greatly improves the survival rate of more severely affected cattle. The carrier state may be eliminated by administration of a long-acting oxytetracycline preparation (20 mg/kg, IM, at least two injections with a 1-week interval). Withholding periods for tetracyclines apply in most countries. Injection into the neck muscle rather than the rump is preferred.
Imidocarb is also highly efficacious against A marginale as a single injection (as the dihydrochloride salt at 1.5 mg/kg, SC, or as imidocarb dipropionate at 3 mg/kg, SC). Elimination of the carrier state requires the use of higher repeated doses of imidocarb (eg, 5 mg/kg, IM or SC, two injections of the dihydrochloride salt 2 weeks apart). Imidocarb is a suspected carcinogen with long withholding periods and is not approved for use in the USA or Europe.
In South Africa, Australia, Israel, and South America, infection with live A centrale (originating from South Africa) has been used as a vaccine to provide cattle with partial protection against the disease caused by A marginale. In the USA, where live vaccines cannot be used, vaccines comprising nonliving A marginale purified from infected bovine erythrocytes and adjuvant have been used in the past but are no longer available. Long-lasting immunity against A marginale is conferred by preimmunization with live rickettsia, combined with the use of chemotherapy to control severe reactions. .Subunit vaccines to control bovine anaplasmosis are under investigation. In some areas, sustained stringent control or elimination of the arthropod vectors may be a viable control strategy; however, in other areas immunization is recommended.
Key Points
Bovine anaplasmosis is endemic in many areas of the world and is transmitted by several tick vectors.
Certain countries use the less pathogenic Anaplasma centrale as a live vaccine, but it has not been used in North America.
Clinical signs include progressive anemia and fever with disease severity age-dependent, because cattle < 1 year old show no or mild clinical signs. Laboratory diagnosis is usually confirmed using stained blood smears and ELISA.
Outbreaks of bovine anaplasmosis are usually seasonal, and tetracyclines and imidocarb are effective treatments.
A ovis causes mild to severe disease in sheep, goats, and deer but is not infectious for cattle.
For More Information





