

Cervical Spondylomyelopathy in Animals
Cervical spondylomyelopathy, also called cervical vertebral malformation-malarticulation and wobbler syndrome, is compression of the spinal cord caused by abnormal development of the cervical vertebrae. Genetic factors and possibly nutrition may be involved.


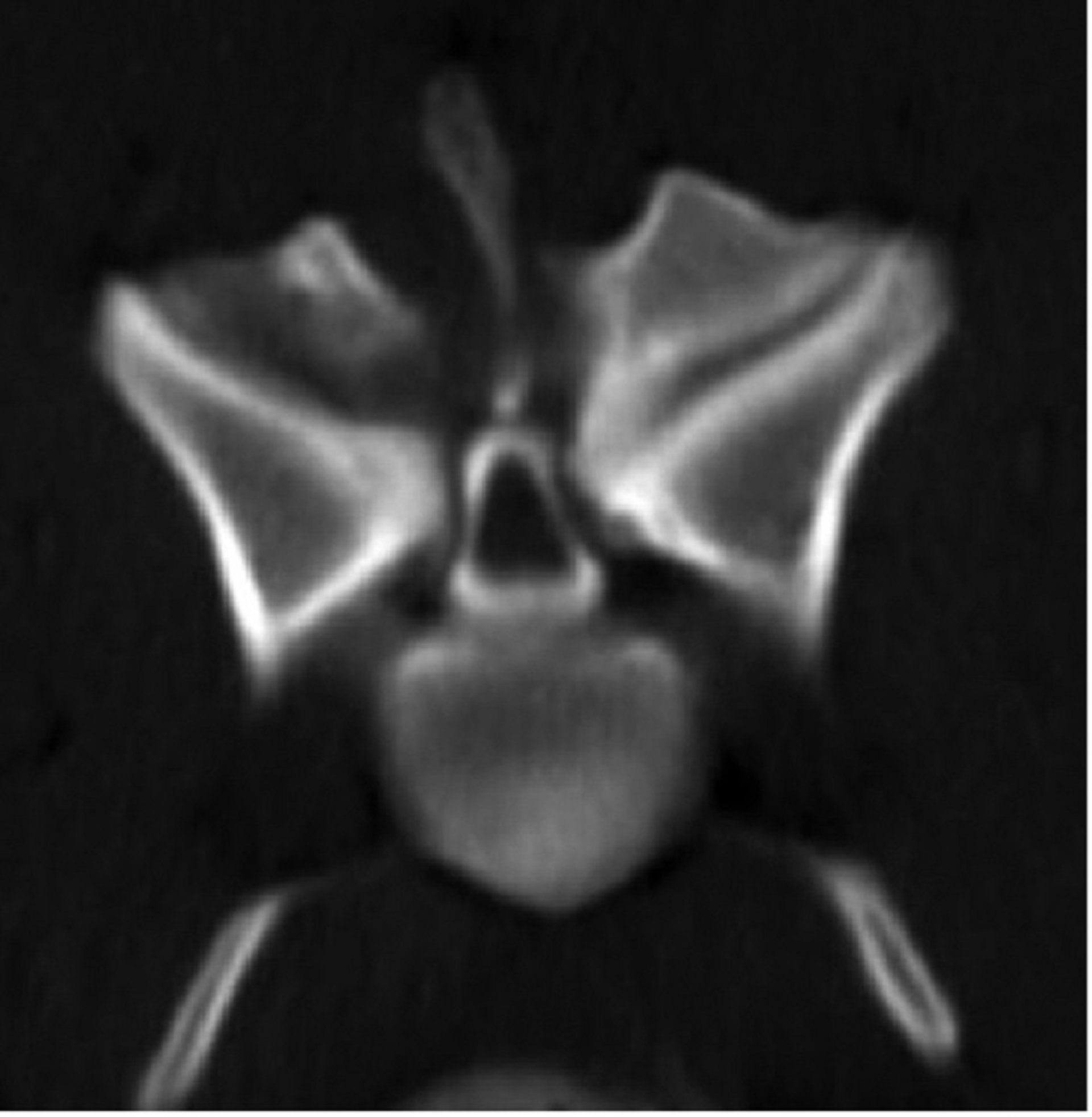
Courtesy of Dr. William Thomas.
In dogs, there are two forms of the disease. Disk-associated wobbler syndrome (DAWS) affects middle-aged large-breed dogs, especially Doberman Pinschers (typical age of onset, 7 years). There is ventral compression of the spinal cord due to protrusion of one or more caudal cervical disks. Some cases are complicated by congenital stenosis of the vertebral canal or hypertrophy of the ligamentum flavum. Bony-associated cervical spondylomyelopathy affects young giant-breed dogs, including Great Danes, Mastiffs, and Rottweilers (age range, several months to 4 years). Spinal cord compression is due to bony proliferation of the articular processes and pedicles, usually of the C4 through C7 vertebrae.

Courtesy of Dr. William Thomas.
Clinical signs of cervical spondylomyelopathy can be acute or slowly progressive. Mild cases are characterized by subtle ataxia of all limbs, often evident as a long, protracted stride in the pelvic limbs, with short-strided gait in the thoracic limbs (sometimes called a two-engine gait). In severe cases, there is paresis or paralysis of all limbs. Neck pain is variable.
Differential diagnoses of cervical spondylomyelopathy include the following:
congenital anomalies
trauma
meningomyelitis
diskospondylitis
neoplasia
Survey radiographs cannot confirm a diagnosis of cervical spondylomyelopathy; however, they are useful in excluding diskospondylitis and bony neoplasia. Definitive diagnosis requires myelography, CT, or MRI.
Nonsurgical treatment of cervical spondylomyelopathy is indicated for dogs with mild clinical signs and consists of exercise restriction, prednisone (0.5 mg/kg, PO, every 24 hours, tapered slowly over months to years), and, if necessary, weight loss. Clinical signs improve in ~50% of dogs and remained unchanged in ~25% of dogs with nonsurgical treatment. Surgery is indicated in animals with substantial neurologic deficits and in those that do not respond adequately to nonsurgical treatment. The specific technique is based on the changes evident on imaging and include ventral slot procedure with partial diskectomy, dorsal laminectomy, distraction and fusion of affected vertebrae, or placement of an artificial disk. Overall, ~80% of dogs do well with surgery.
In horses, cervical spondylomyelopathy is the most common noninfectious disease of the spinal cord and occurs in many breeds. Most horses present at <3 years of age, although they can be affected at any age. The mid-cervical region is most commonly affected, and there is proprioceptive ataxia and tetraparesis. Diagnosis is based on imaging and excluding other causes. Plain radiographs may show abnormal articular facets and stenosis of the vertebral canal. Myelography is necessary for definitive diagnosis and surgical planning. Nonsurgical treatment involves NSAIDs and dimethyl sulfoxide to reduce inflammation. In yearlings, diet modification can help. Surgery most commonly involves ventral fusion of the affected vertebrae. Approximately 80% of affected horses improve with surgery. Handler and rider safety is a major concern in horses with ataxia.
Degenerative Lumbosacral Stenosis in Animals

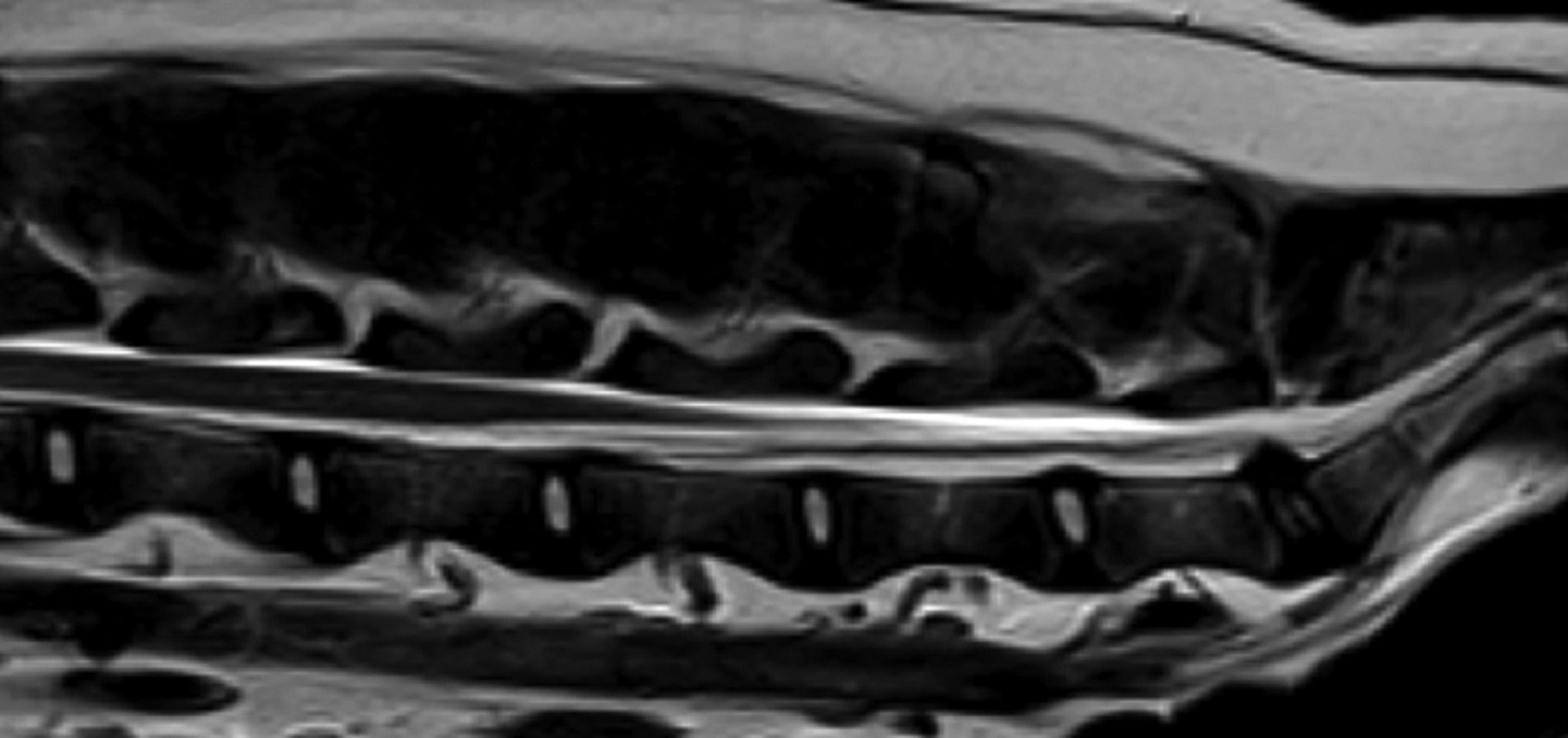
Photo courtesy of Dr. William Thomas.
Narrowing of the lumbosacral vertebral canal or intervertebral foramina results in compression of the cauda equina or nerve roots. It is most common in large breeds of dogs, especially German Shepherd Dogs, and is rare in cats. It results from degeneration and protrusion of the L7–S1 disk, hypertrophy of the ligamentum flavum, or rarely subluxation of the lumbosacral joint. The cause is unknown, although German Shepherd Dogs with congenital transitional vertebrae are at increased risk. Clinical signs typically begin at 3–7 years of age and may include difficulty using the pelvic limbs, pelvic limb lameness, tail weakness, and incontinence. Pain on palpation or extension of the lumbosacral joint is the most consistent finding. There may be proprioceptive deficits, muscle atrophy, or a weak flexor reflex in the pelvic limbs.
Plain radiographs may show degenerative changes; definitive diagnosis, however, requires MRI, CT, or epidurography. Dogs in which mild pain is the only clinical sign may improve with 4–6 weeks of rest. Epidural injection of methylprednisolone acetate (1 mg/kg on each of day 1, day 14, and day 42) is effective in ~80% of dogs with pain and minimal neurologic deficits. Surgery is indicated when pain is refractory to medical treatment or there are neurologic deficits. The most common surgical technique is dorsal laminectomy with partial diskectomy; however, foramenotomy or stabilization is indicated in certain cases. Approximately 70%–95% of dogs improve with surgery, although preexisting urinary incontinence may not resolve.
Degenerative Myelopathy in Dogs
Degenerative myelopathy of dogs, also called chronic degenerative radiculomyelopathy, is a slowly progressive, noninflammatory degeneration of the axons and myelin primarily affecting the white matter of the spinal cord. It is most common in German Shepherd Dogs, Pembroke Welsh Corgis, Boxers, Rhodesian Ridgebacks, and Chesapeake Bay Retrievers; however, it is occasionally recognized in many other breeds. The cause is a mutation in the superoxide dismutase 1 (SOD1) gene, inherited in an autosomal recessive pattern with incomplete penetrance. It is similar to familial amyotrophic lateral sclerosis in human patients. Pathologically, there is noninflammatory degeneration of axons in the white matter of the spinal cord, which is most severe in the thoracic region.
Affected dogs are usually >8 years old and develop an insidious onset of nonpainful ataxia and weakness of the pelvic limbs. Spinal reflexes are usually normal or exaggerated; in advanced cases, however, there is flaccid tetraparesis and hyporeflexia reflecting lower motor neuron involvement. Early cases may be confused with orthopedic disorders; however, proprioceptive deficits are an early feature of degenerative myelopathy and are not evident in orthopedic disease.
Myelography or MRI and CSF analysis are essential to exclude compressive and inflammatory diseases. A DNA test based on the SOD1 gene is available on the Orthopedic Foundation for Animals Web site. Dogs that are homozygous for the mutation are at risk of the disease and will pass one copy of the mutant allele to their offspring. Heterozygotes are at low risk of the disease; however, they have a 50% chance of passing one copy of the mutant allele to each offspring. Homozygous normals are at low risk of the disease and will not pass the mutation to offspring.
There is no specific treatment of degenerative myelopathy and no evidence that glucocorticoids, other drugs, or supplements alter the course of the disease. Most dogs are euthanized because of disability within 1–3 years after diagnosis.
Degenerative Myeloencephalopathy in Horses
Equine degenerative myeloencephalopathy, also called equine neuroaxonal dystrophy, is a progressive neurologic disorder of horses and zebras characterized by diffuse degeneration of axons, myelin, and neurons in the spinal cord and, to a lesser extent, the brainstem. It has been reported in many equine breeds in North America, Australia, and England. The cause is incompletely understood; however, a vitamin E deficiency and genetic factors are likely.
Clinical signs of equine degenerative myeloencephalopathy usually become apparent during the first year of life and consist of ataxia and weakness in all four limbs, although the pelvic limbs may be more severely affected. Clinical signs may stabilize or slowly progress.
There is no definitive diagnostic test. Clinical diagnosis is based on clinical features and excluding other causes. Results of myelography and CSF analysis are normal.
Preventive measures include ensuring access to lush, green pasture for mares and for young horses up to 2 years old. Supplementation of pregnant mares and newborn foals with vitamin E is preventive in predisposed families. Serum alpha-tocopherol concentrations of the dam can determine the need for supplementation during pregnancy and lactation. For foals, the serum alpha-tocopherol concentration should be evaluated within the first week of life to determine the need for supplementation. Once neurologic signs develop, supplementation can prevent worsening; however, it does not reverse neurologic deficits.
Intervertebral Disk Disease in Animals
Degeneration and subsequent herniation of the intervertebral disk results in compression of the spinal cord, spinal nerve, or nerve root. It is a common cause of spinal cord disease in dogs, with a lifetime prevalence of ~3.5%. Clinical signs of disk disease are rare in cats and horses. Chondrodystrophoid breeds of dogs (eg, Dachshund, French Bulldog, Beagle, Shih Tzu, Lhasa Apso, and Pekingese) are most commonly affected, with Miniature Dachshunds having a lifetime prevalence of ~20%. In these breeds, there is chondroid degeneration of the disks within the first few months of life. Disk extrusion can occur as early as 1–2 years of age, and clinical signs are often acute and severe. Two fibroblast growth factor 4 (FGF4) retrogenes—one on Canis familiaris chromosome (CFA) 18 and one on CFA 12—contribute to the chondrodystrophoid phenotype, with the FGF4 on CFA 12 drastically increasing the risk of disk degeneration.

Courtesy of Dr. William Thomas.
Large-breed dogs can suffer fibroid disk degeneration as they age. This type of degeneration predisposes to a slowly progressive protrusion of the disk. Clinical signs of intervertebral disk disease typically develop at >5 years old and consist of slowly progressive ataxia and paresis.

Courtesy of Dr. William Thomas.
A third type of intervertebral disk herniation is acute extrusion of a healthy, nondegenerate disk. It occurs most commonly during exercise in relatively young dogs. In some cases the extruded disk material compresses the spinal cord or even penetrates the dura mater or spinal cord. In other cases, the volume of extruded disk material is so small that it does not cause any persistent compression; however, the velocity of extrusion causes a concussive injury to the spinal cord, a syndrome referred to as acute noncompressive nucleus pulposus extrusion (ANNPE).
The most common sites of disk herniation are the cervical and thoracolumbar regions. The predominant clinical sign of cervical disk herniation is neck pain, manifested as cervical rigidity and muscle spasms. There may be thoracic limb lameness (nerve root signature) or neurologic deficits, ranging from mild tetraparesis to tetraplegia.
In thoracolumbar disk herniation, there may be back pain, evident as kyphosis and reluctance to move. Neurologic deficits are usually more severe than those that occur in cervical disk disease and range from pelvic limb ataxia to paraplegia and incontinence. In paraplegic animals, the most important prognostic finding is whether there is deep pain perception caudal to the lesion. This is assessed by pinching the toe or tail and observing whether there is a behavioral response, such as a bark or turn of the head. It is important to pinch the bone to stimulate deep pain receptors, not just the skin, which tests only superficial pain. Reflex flexion of the limb must not be mistaken for a behavioral response.
Definitive diagnosis of disk extrusion is based on imaging studies. Spinal radiographs may show narrowing of the affected disk space, intervertebral foramen or articular facets, or radiodense calcified disk material within the vertebral canal. However, radiographs are not sensitive or specific enough for definitive diagnosis, which requires myelography, MRI, or CT. Dogs with pain and minimal to moderate neurologic deficits often recover with 2–3 weeks of cage rest. A short course of prednisone (0.5 mg/kg, PO, every 24 hours for 3 days) is often helpful in relieving pain; however, there is no evidence that steroids or any other drugs improve neurologic recovery. The use of anti-inflammatory or analgesic medication without concurrent cage rest is contraindicated because an increase in the dog’s activity may lead to further disk extrusion and worsening of spinal cord compression. Clinical signs recur after conservative treatment in 30%–40% of cases.
Recovery Rates After Surgery for Intervertebral Disk Disease in Dogs
Patient Type | Recovery Rate |
|---|---|
Nonambulatory small-breed dog with thoracolumbar extrusion and intact deep pain | 85%–95% |
Small-breed dog with thoracolumbar extrusion and loss of deep pain < 24 hours | 50% |
Small-breed dog with thoracolumbar extrusion and loss of deep pain >24 hours | < 50% |
Nonambulatory large-breed dog with chronic thoracolumbar protrusion | 25%–50% |
Ambulatory dog with cervical disk disease | 95% |
Nonambulatory dog with cervical disk disease | 65%–95% |
In animals with severe neurologic deficits, prompt surgery offers the best chance of recovery in patients with appreciable spinal cord compression ( Recovery Rates After Surgery for Intervertebral Disk Disease in Dogs). Other indications for surgery to treat intervertebral disk disease are failure of conservative treatment and recurrent episodes. For cervical disk extrusion, a ventral slot procedure is the most common. Hemilaminectomy with removal of the extruded disk material is the most common procedure for thoracic or lumbar extrusions. Prophylactic fenestration of commonly affected disk spaces (eg, T11 through L4) decreases recurrence in small-breed dogs. Progressive myelomalacia develops in 5%–10% of dogs with paraplegia and loss of deep pain perception. In this syndrome, affected dogs develop flaccid tetraplegia, the level of anesthesia ascends cranially, and respiratory paralysis develops.
Diffuse Idiopathic Skeletal Hyperostosis in Dogs


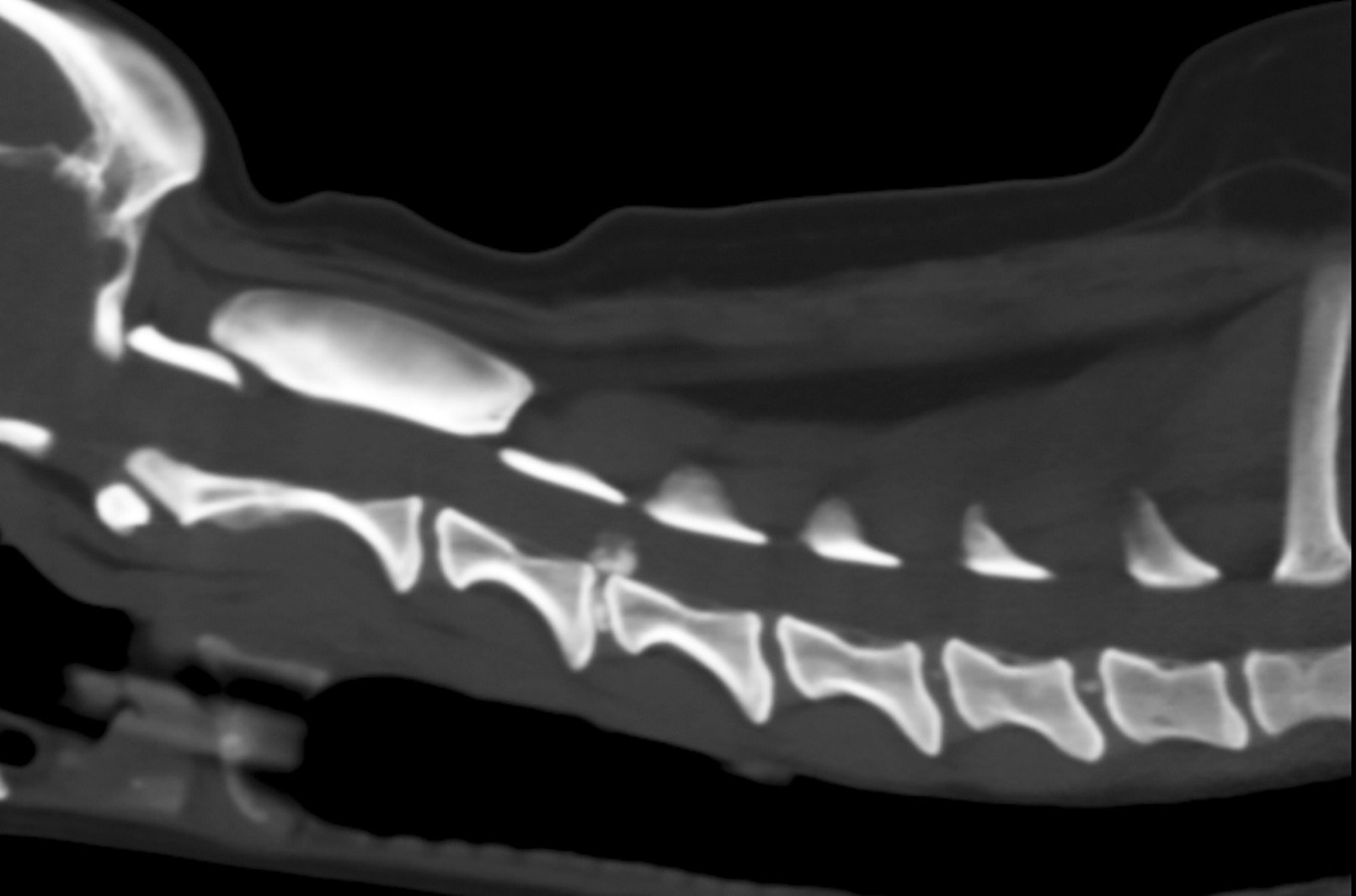
Courtesy of Dr. William Thomas.
Also known as Forestier disease in human patients, diffuse idiopathic skeletal hyperostosis (DISH) is characterized by ossification of entheses, the sites where a ligament, tendon, or joint capsule inserts into bone. Radiographic criteria for diagnosis are flowing ossification along the ventrolateral aspect of at least four contiguous vertebrae with relative preservation of disk width and absence of facet joint ankylosis. Approximately 4% of dogs >1 year old are affected, and prevalence increases with age. As with spondylosis deformans, Boxers are at increased risk, with a prevalence of ~40%. The thoracic and lumbar regions are most commonly affected. It is unclear how often DISH causes clinical signs, and in many cases the radiographic findings are incidental. However, spinal pain and stiffness is possible and, in those cases, treatment involves analgesics as needed.
Motor Neuron Disease in Horses
Equine motor neuron disease is a progressive, noninflammatory degeneration of motor neurons in the spinal cord and brainstem of horses. It is most common in the northeastern US; however, it has been reported in several areas of North and South America, Europe, and Japan. The cause is uncertain, but vitamin E deficiency is a strong risk factor. Adult horses of any age and breed can be affected, although Quarter Horses are affected most commonly. Affected horses typically do not have access to pasture grass and are fed poor-quality grass hay.
Clinical signs of equine motor neuron disease consist of generalized symmetric weakness, trembling, and muscle atrophy. Affected horses often stand with their head held low and their feet camped under their body, frequently shifting their weight from one limb to another. Ataxia is not a feature of this disease, in contrast to most spinal cord diseases. Many affected horses have retinal abnormalities, including a distinct reticulated pigment pattern and areas of hyperreflectivity. Electromyography and biopsy of the spinal accessory nerve or the sacrodorsalis caudalis muscle are useful in diagnosis.
There is no specific treatment for equine motor neuron disease; however, some horses improve partially after 2–3 months of illness. Horses that lack access to green forage high in vitamin E for prolonged periods should be supplemented with vitamin E.
Degeneration of Motor Neurons in Animals
Degeneration of motor neurons is an inherited or sporadic disease that occurs in Brittany Spaniels, Pointers, German Shepherd Dogs, Doberman Pinschers, and Rottweilers; cats; Hereford, Brown Swiss, and red Danish cattle; Yorkshire pigs; and goats. Also called spinal muscular atrophy, this disease is characterized by progressive paresis, tremor, muscle atrophy, and weak spinal reflexes. The age of onset is typically within the first 1−2 years of life. Electromyography and muscle biopsy help document muscle denervation; definitive diagnosis, however, is based on loss of motor neurons in the ventral horn of the spinal cord and brainstem nuclei on necropsy.
Metabolic Storage Disorders in Animals
Rare, usually inherited, metabolic disorders can affect the CNS, including the spinal cord. (Also see Congenital and Inherited Anomalies of the Nervous System in Small Animals.)
Spondylosis Deformans in Animals


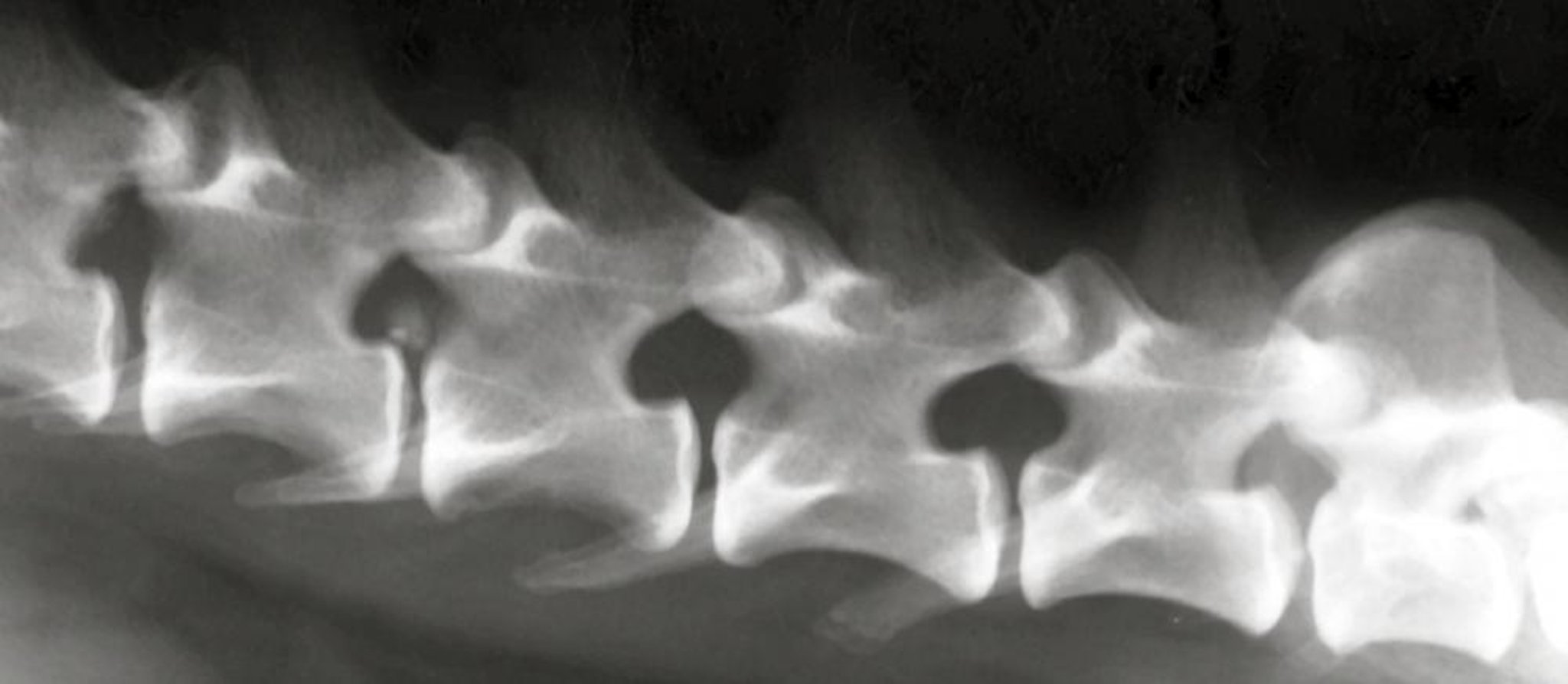
Courtesy of Dr. William Thomas.
Spondylosis deformans is a noninflammatory condition characterized by formation of bony projections (enthesophytes) at the location where the annulus fibrosus is attached to the cortical surface of adjacent vertebrae. These bony growths vary from small spurs located several millimeters from the junction between the disk and vertebra to bony bridges that span the disk space, leaving at least part of the ventral surface of the vertebra unaffected. The enthesophytes typically expand laterally and ventrally but not dorsally; therefore, they rarely affect the spinal cord. The cause is breakdown of the outer fibers of the annulus fibrosis and stretching of the longitudinal ligament. The increased stress at the vertebral attachment of the longitudinal ligament incites bony production.
Spondylosis deformans occurs in dogs, cats, and bulls, and the incidence increases with age. It is uncommon in dogs <2 years old; by 9 years of age, 25%–70% of all dogs are affected. It is especially common in Boxers, and a genetic predisposition has been identified in this breed. It is typically an incidental radiographic finding, and there is no correlation between the presence of spondylosis and clinical signs. Rare cases cause spinal hyperesthesia, which should be treated with analgesics.





