



Whenever possible, elimination of a tumor by surgery is preferred and often carries the greatest likelihood of cure. However, in many instances, large neoplasms, or those in critical areas such as the brain, are not amenable to complete or even partial surgical removal. Even when a tumor is grossly removed, microscopic foci of neoplastic cells often extend beyond the limits of the surgical field. This is more common for some tumor types than for others. In all of these instances, radiation therapy, often in combination with chemotherapy, is efficacious in treating cancer.
Radiation therapy is the treatment of choice for most brain tumors, nasal tumors, and other neoplasms of the head and neck where even partial resection may be extremely disfiguring or carries a high risk of mortality and minimal or no chance for control. It may be the only treatment option for cancer of the vertebral column and pelvic canal.
Radiotherapy is also used to treat tumors in the mediastinum and soft tissues of the skin and subcutis either before or after surgery. It is seldom used in veterinary medicine for the treatment of lung neoplasia or in the treatment of neoplastic disease of the upper abdominal cavity, due to the mobility of tumors in these areas. However, treatment of mediastinal cancers and those of the caudal abdomen and pelvic canal, such as thymoma, prostatic carcinoma, and anal gland tumors, are possible and often indicated. As the sophistication of radiotherapy techniques increases, more and more types of neoplasia are being treated at least in part by radiation therapy.
The demand for radiation therapy in veterinary medicine continues to increase, partially due to the continued increase in sophistication of treatment techniques in recent years. A board specialty in radiation oncology recognized by the AVMA is granted by the American College of Veterinary Radiology. The sophistication and scope of both veterinary imaging and radiation therapy has advanced to the point that very few radiologists now actively practice in both the fields of imaging and therapy.
Historically, radiation therapy was delivered using orthovoltage x-ray machines or very large activities of cobalt-60 and cesium-137. Except for a few specialized instances, orthovoltage x-ray machines have fallen from favor because of the intensity of adverse radiation reactions associated with their use and their limited flexibility. Cobalt and cesium are no longer used because as long-lived isotopes they are extremely dangerous and heavily regulated in most of the world. Today, it is virtually impossible to purchase these sources because of public safety concerns.
Therapeutic radiation treatments may be delivered in one of three general ways. By far, the most commonly used is external beam radiotherapy (teletherapy), which uses a large external source of radiation to deliver a beam of high-energy radiation selectively to a tumor or tumors that have been delineated using some form of imaging (usually computed tomography). The second method of delivering radiation therapy is brachytherapy, which uses much smaller radiation sources applied directly to or implanted within the tumor. The implantation or application of these sources may either be permanent or temporary. The third way in which radiation therapy may be used blurs the lines between radiation therapy and nuclear medicine and involves the administration of a radioactive therapeutic agent to a patient and having the radioisotope localize within the tumor by one of a variety of physiologic processes. This has sometimes been referred to a nuclear oncology or biologically targeted radiotherapy.
Teletherapy in Animals
Veterinary radiation therapy practices today almost exclusively use linear accelerators as the source of the ionizing radiation used to treat neoplasia and occasionally specific benign diseases. These machines produce powerful x-rays and electron beams with energies of 4–20 million electron volts. The x-rays are used to treat deep-seated tumors, whereas electron beams are generally used to treat tumors of the skin and subcutis. Linear accelerators are complex machines that require the support of a medical physicist to maintain safe and effective use. This increased support load is offset by the machine’s flexibility and speed, which is necessary as treatment techniques become more sophisticated and complex. The lack of need for periodic replacement of cesium-137 and cobalt-60 sources is another significant advantage.
Computerized treatment planning systems that accurately model the deposition of radiation energy within the body are used by veterinary radiation oncologists to improve the localization and distribution of the therapeutic beam within the patient. This reduces the dose to normal tissues relative to the dose delivered to neoplastic tissue, improving control rates while reducing the severity of normal tissue complications. These programs are used in conjunction with CT or MRI images, which determine the position and extent of the tumor within the body and its position in relation to normal structures.
Hours of work on the computer by a radiation oncologist or dosimetrist may be required to carefully delineate the tumor and each of the normal structures at risk to generate a treatment plan for a large, complex tumor. The computer system is able to quickly generate dose profiles for proposed treatment configurations and determine whether the plan meets certain treatment constraints set by the radiation oncologist.
Once the treatment plan is set, the patient is then treated in precisely the same position they were in for the CT or MRI. Repeatability of positioning is of paramount importance, and special positioning devices are used in conjunction with careful land-marking to achieve this. This requires that the patient be scanned in exactly the same position in which it will be treated, requiring close communication between the diagnostic and therapeutic radiologists.
To achieve this, a CT is performed with the patient set up in the exact position in which they will be treated. Proper patient positioning is then confirmed using an imaging system integrated with the linear accelerator before a treatment is begun. Once proper positioning is confirmed, the treatment can be administered. Close attention to detail is necessary during this part of the process, because even small changes in position can have profound effects on the distribution of the radiation dose delivered. This is especially true in central nervous system tumors, where the lesion diameter may only be on the order of 1 cm or less.
Except in rare instances, all radiation therapy treatments using external sources of radiation must be delivered with the patient immobilized by general anesthesia. Because the plane of anesthesia required is light and the procedures are typically of a relatively short duration, this repeated anesthesia is well tolerated, and complications are few with proper observation and monitoring by trained and experienced technologists. This requirement for anesthesia is rarely if ever a contraindication for implementing a course of radiation therapy.
A typical course of radiation therapy consists of multiple doses of radiation delivered on different days. This is done to allow healthy tissues to heal somewhat between doses. Healthy tissues have a greater ability to repair radiation damage than neoplastic tissues; therefore, use of multiple, small doses of radiation, which have a cumulative effect, favors survival of healthy over neoplastic tissues.
Most radiation therapy regimens designed with curative intent use 15–20 individual doses (fractions) of radiation. Each dose of radiation may be delivered using several different beams of radiation of differing size, shape, and intensity. IMRT, or intensity modulated radiation therapy, is a newer adaptation of radiation therapy in which each of the primary radiation treatment beams is broken down into a number of smaller beams to tightly control the deposition of radiation injury in the tissue, thereby improving not only tumor control but normal tissue complication rates.

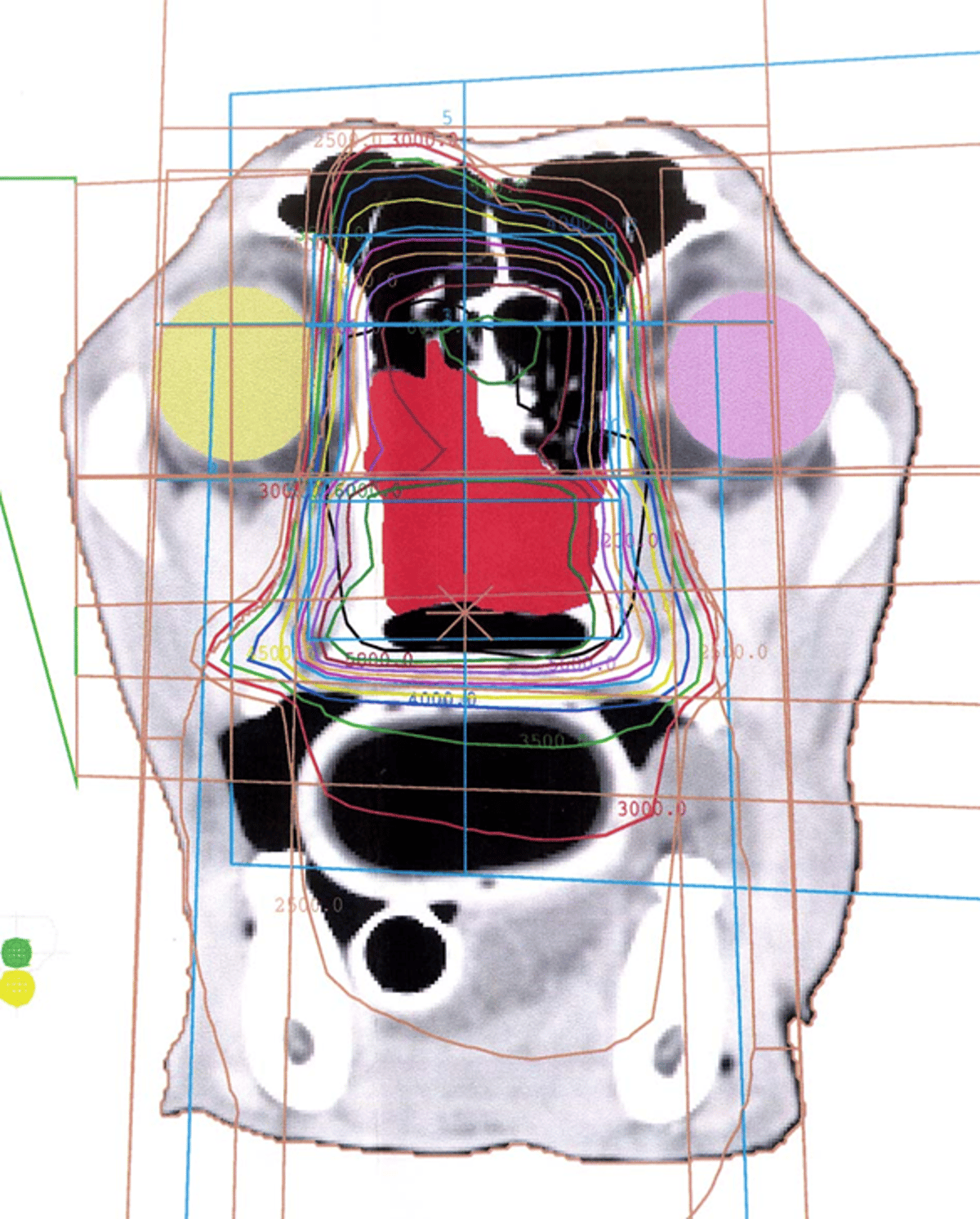
Courtesy of Dr. Jim Lattimer.

Courtesy of Dr. Jim Lattimer.

Courtesy of Dr. Jim Lattimer.
In the past decade, another dimension of external beam radiation therapy has been developing. This is referred to as stereotactic radiosurgery (SRS) or stereotactic body radiation therapy. In this type of radiation therapy, a curative, intense dose of radiation therapy is delivered to the tumor in 1–4 treatments on consecutive or alternating days in a single week. This markedly reduces the hospital stay for the patient and the inconvenience for the owner, but often not the cost.
There are many constraints to the use of this type of radiation therapy protocol. The radiation doses used are quite high per dose and for the time period over which the treatments are given. This requires extreme precision in the administration of the radiation beam to avoid normal tissues and to irradiate only the neoplastic tissue. To achieve this precision requires not only the ability to perform IMRT-type radiation administration but the ability to modify the treatment plan at each fraction and monitor the delivery of the radiation dose in real time while the radiation is being administered. The equipment required to do this is both delicate and expensive.
Although SRS has a number of advantages, it also has the potential to result in severe normal tissue side effects if an inappropriate administration occurs or if large amounts of tumor undergo acute necrosis. For these and a number of other reasons related to the physics of radiation, SRS may not be appropriate for large tumors (>4 cm in diameter), especially if the tumor is located in a high-risk anatomic area such as the throat.
In cases where the tumor is too advanced to be controlled by radiation, palliative therapy with larger doses and fewer fractions of radiation may be used to retard the tumor's growth or reduce associated pain. This is done to improve the patient’s quality of life or to give the owner more time with their animal. Palliative protocols are not intended to be curative but therapeutic. This is an essential difference between SRS and palliative protocols. Palliative protocols have much lower dose intensity than SRS. Such a palliative approach may also be used when mandated by owner finances. Such treatments have a low likelihood of resulting in durable control of the cancer, and they carry a greater risk for late radiation effects if a durable control does occur, which happens in a quite small percentage of cases.
Radiation therapy, even when combined with surgery and chemotherapy, may not be curative. However, it can delay the development or expansion of disease in many instances. Radiation oncologists typically speak in terms of control rate rather than cure. Sometimes, the control may be relatively short lived, and recrudescence of the tumor occurs within months after completion of the treatment regimen. In other cases, control may last several years or even until another disease supersedes the neoplasia. Unfortunately, it is seldom possible to predict even within an individual tumor type which patients will experience good control and which ones will not. Continual advances in the evaluation of genetic markers within tumors hold the promise of being able to better predict control in the future.
Because of the risk of serious and potentially life-threatening complications associated with this treatment modality, the complexity of the equipment and sophistication of the radiation therapy procedures, radiation therapy should only be prescribed by and administered under the supervision of a veterinarian with special training, experience, and certification in the field of veterinary radiation oncology. A veterinary radiation oncologist should also be consulted any time further treatment is contemplated for neoplasia that has been treated by radiation therapy. This is particularly important if surgery within the radiation field is being considered.
Brachytherapy in Animals
Brachytherapy is the implantation of radioactive sources into the tumor to achieve radiation therapy. It is widely used in human medicine, but seldom for treatment of cancers in animals because of the difficulties associated with maintenance of the sources and keeping the sources in place within the tumor. Radiation safety is also a concern in that the patients must be monitored and confined until the sources are removed or decay to a nonradioactive state. However, implantation of the radiation source directly into the tumor results in very high doses of radiation to the tumor with minimal dose to surrounding tissue. This can improve the control rate in many instances, with a reduction in normal tissue complications as compared with external beam radiation therapy.
Brachytherapy treatment times are on par with those seen with SRS and results may be similar. The implantation of the sources is, however, a surgical procedure and carries with it some degree of risk. One of the major barriers to use of this type of treatment is cost, in that the sources are expensive to purchase and maintain and may require frequent replacement or even be single use if they are to be a permanent implant.
Implantable radiation sources that are so small (microns or even nanometers) that they are permanently implanted within the body blur the margins between radiation therapy and nuclear medicine. The implantation of such sources comes under the heading interventional radiology. Interventional radiology procedures such as catheter placement and CT guidance of source implantation are used to introduce both macroscopic and microscopic scale brachytherapy sources into neoplasms located deep within the body. Targeting of such agents is accomplished either by using sources of sufficient size to be locally retained within the tissue or capillaries of the tumor or by targeting them specifically to tumor cells using monoclonal antibody labeling.
These techniques have been around for many years but have not received widespread attention in veterinary medicine because of the cost of both the agents and the equipment required for their implantation. However, in recent years there has been a marked upswing in the interest in such interventional radiology procedures for both treatment and diagnosis, not only of cancer but also of many other conditions. Such techniques may well increase the interest in and availability of brachytherapy procedures. Because of the risk of excessive radiation exposure and contamination of the patient or hospital, these procedures should be performed only by veterinarians with appropriate training, experience, and support in a properly licensed facility.
Biologically Targeted Radiotherapy in Animals
Although the concept of biologically targeting treatment agents such as radioisotopes has been considered for decades, it has been little used in medical practice in either human or veterinary medicine until recent years. The notable exception to this is the use of radioiodine to treat thyroid cancers in both human and veterinary patients. In veterinary medicine, this has become a mainstay of treatment of thyroid adenomas in cats and occasionally to treat thyroid adenocarcinomas in dogs. When deemed appropriate by pretreatment testing, this can be a very effective and efficient way to treat these conditions in animals.
Bone-seeking radioisotopes developed for treatment of metastatic osseous neoplasia in humans are also useful in the treatment of primary and metastatic bone cancer in dogs and cats. Cancer-seeking mononuclear antibody and small-molecule isotope carriers are currently available for treatment of a variety of neoplasias in humans, such as neuroendocrine and mammary carcinomas. More agents of this type are regularly being introduced, and it is reasonable to believe they may become the dominant form of radiation therapy in the future. Such nuclear oncology treatments are in some instances directly applicable to veterinary patients as well. In the usual course of events, these treatments are often tested in veterinary patients before being introduced into human medicine.
Biologically targeted radiotherapy may also be effective in the treatment of metastasis distant from the primary tumor, which is another advantage over conventional radiation therapy in which the treatment of metastasis is usually limited to treatment of regional lymph nodes or, in rare occasions, up to 3 distant metastases. As the number of agents grows, more tumor types may potentially be treated in this way.
Radiation Therapy Results and Side Effects in Animals
Regardless of the way in which the radiation is delivered, the goal of radiation therapy is to eradicate or severely damage the tumor cells to prevent further growth or regrowth of the tumor cells. It is inevitable that some normal cells and tissues will be irradiated at the same time, and it is the damage to these normal structures that limits the radiation dose that can be delivered.
There is often a very fine line between the dose that will control the tumor and the dose that the normal tissues can tolerate or recover from. The way radiation therapy is currently practiced, there is almost always a therapeutic effect on the tumor. This results in either tumor regression or cessation of growth that lasts for a variable period of time. Side effects on normal tissues are frequent , and can occur either immediately after the radiation therapy or later. The short-term side effects are managed medically and, unless very severe, generally heal 4–6 weeks after the end of the course of treatment. The later effects may result in loss of function and fibrosis or even necrosis of normal tissues, and these are the effects that dictate the design of radiation therapy plans. With careful planning and management of normal tissue side effects, nearly all radiation therapy patients will have a positive effect of varying duration.
The radiosensitivity of virtually any neoplasm is higher in minimal or microscopic disease. Some neoplasms respond well initially but tend to recur at some time after radiation therapy. The time to recrudescence is highly variable between and within tumor types.
A full list of appropriately trained and accredited veterinarians as well as a list of radiation therapy facilities can be obtained through the American College of Veterinary Radiology. More information on the management of cancer in general is available from the Veterinary Cancer Society.
For More Information
Also see pet health content regarding radiation therapy.




