

Chronic indigestion (or vagal indigestion) syndrome refers to functional or mechanical disturbances of the ruminant stomach that impair gastrointestinal transit. Clinical signs include abdominal and ruminal distension as well as poor appetite, weight loss, dehydration, reduced fecal output, and bradycardia. Treatment depends on the underlying cause.
Chronic indigestion syndrome (also known as vagal indigestion) is characterized by the gradual development of abdominal distention secondary to ruminoreticular distention. In addition to vagal nerve damage, several other factors may contribute to the development of this condition. Clinically, proximal (reticulo-omasal) functional stenosis is distinguished from distal (pyloric) functional stenosis. Abdominal distension is characteristic of both forms and results in a characteristic abdominal contour described as papple-shaped (ie, apple-shaped on the left and pear-shaped on the right when the animal is viewed from behind). Impaired passage of ingesta results in rumen distention, and palpation reveals ruminal contents with a soft to liquid consistency. Clinical findings can support a tentative diagnosis, and the measurement of rumen chloride concentration aids in the differentiation of proximal and distal stenosis. Ultrasonographic evaluation of the abdomen may identify the cause of the disease. The prognosis is grave in cases without an etiologic diagnosis, and guarded when a specific cause, such as traumatic reticuloperitonitis or liver abscess, can be identified and treated successfully.
Etiology and Pathogenesis of Chronic Indigestion Syndrome in Ruminants
Chronic indigestion was previously believed to be the result of vagal nerve damage due to traumatic reticuloperitonitis, but several other causes have been identified. Vagal indigestion is also known as Hoflund syndrome, in recognition of Sven Hoflund, who in 1940 first described the condition. Historically, the disease was divided into types I–IV; for clinical purposes, however, it is sufficient to distinguish between proximal (reticulo-omasal) and distal (pyloric) stenosis. The term functional stenosis is commonly used because in most cases there is no narrowing, stricture, or mechanical obstruction of the passage. With proximal functional stenosis, the passage of ingesta from the ruminoreticulum to the omasum and abomasum is impaired, resulting in rumen overload. With distal functional stenosis, abomasal emptying is impaired, leading to abomasal overload and reflux of abomasal contents into the omasum and ruminoreticulum.
Vagal nerve damage can occur in the cranial abdomen in animals with reticuloperitonitis and in the pharyngeal region after an injury. Periesophagitis, paraesophageal abscess, or megaesophagus can lead to vagal nerve damage in the esophageal region, and enlargement of the mediastinal lymph nodes associated with bronchopneumonia or neoplasia can result in nerve impairment in the thoracic region. Vagal nerve lesions can occur distal to the reticulum—in cattle with right displaced abomasum (RDA) or abomasal volvulus, for instance—especially when surgical correction is delayed. Such cases are referred to as gastrointestinal dysfunction resembling vagal indigestion (GDRVI), and affected cattle develop vagal indigestion within 5 days after surgery. In addition to damaging the vagal nerve, lesions of the abomasal wall or peritonitis can cause vagal indigestion.
Other causes that are not associated with vagal nerve damage include mechanical impairment of reticular and ruminal motility resulting from adhesions and abscesses, and they are most likely associated with pressure due to these lesions. Enlargement of the uterus in late gestation can mechanically limit the intestines, leading to inhibition of abomasal emptying with subsequent abomasal distention, particularly in the presence of adhesions of the forestomachs and abomasum. Finally, in rare cases, the reticulo-omasal orifice, the esophageal groove, or the cardia may become obstructed by materials (eg, bits of rope, pieces of placenta, or bezoars) or by fibromas, papillomas, abscesses, or actinomycetomas.
Clinical Findings of Chronic Indigestion Syndrome in Ruminants


Abdominal dilatation, as viewed from behind, in a 9-year-old Brown Swiss cow with chronic indigestion attributable to an abscess involving the reticulum and liver.
Courtesy of Dr. Ueli Braun.
The clinical signs of proximal and distal functional stenosis are similar; they tend to be chronic and characterized by progressive anorexia and weight loss in cattle with proximal stenosis. With distal stenosis, however, they are often acute and manifest clinically within a few days. Abdominal enlargement and distention occur in both forms. When viewed from behind, the abdominal contour is apple-shaped on the left and pear-shaped on the right, giving rise to the term papple, derived from pear and apple. The rumen may become overloaded and distended due to impaired passage of ingesta, and failure of eructation may lead to tympany. The rumen contents are no longer stratified; instead they are uniform, and on transabdominal palpation they have a mushy to watery consistency. Rumen motility may be normal, decreased, or increased. Reticular hypermotility is often detected on ultrasonographic examination. Transrectal palpation reveals an L-shaped rumen because the enlarged ventral sac extends far to the right. Fecal output is decreased, and the feces may contain large particles, measuring 2 to 4 cm. Other clinical signs are bradycardia, dull coat, partial or complete absence of rumination, and hypothermia. In cattle with distal functional stenosis, health status may deteriorate quickly because of abomasal reflux syndrome.
Diagnosis of Chronic Indigestion Syndrome in Ruminants
Clinical findings for tentative diagnosis
Atropine test for cattle with bradycardia
Measurement of rumen chloride concentration to differentiate between proximal and distal functional stenosis
A tentative diagnosis of proximal or distal functional stenosis is based on clinical findings. Bradycardia with an increase in heart rate of >16% in response to the subcutaneous administration of 40 mg atropine sulfate is suggestive and has a diagnostic certainty of 98% for a permanent vagal nerve lesion. The rumen chloride concentration enables differentiation of proximal and distal functional stenosis, and lesions causing vagal nerve damage may be identified by ultrasonographic examination. Exploratory laparotomy reveals ruminoreticular dilatation in cattle with proximal functional stenosis, and dilatation of the abomasum, omasum, and rumen in cattle with distal functional stenosis.
Laboratory Findings
Laboratory findings of proximal functional stenosis are nonspecific. Total protein and fibrinogen concentrations are increased. The glutaraldehyde test can be used to differentiate chronic from acute inflammatory disease; when stenosis is the result of chronic inflammation, time to clot formation is decreased on the glutaraldehyde test. Distal stenosis is associated with abomasal reflux syndrome and therefore characterized by an increase in the rumen chloride concentration, hypochloremia, hypokalemia, metabolic alkalosis, hemoconcentration, and prerenal azotemia. Rumen chloride concentration is used to differentiate proximal stenosis (mean, 20 mmol/L) and distal stenosis (mean, 57 mmol/L).
The so-called atropine test is indicated in cattle with chronic indigestion and a heart rate of < 60 beats/min. Atropine inhibits the effect of vagal stimulation on the heart and can therefore be used to determine whether bradycardia is vagally mediated or due to cardiac disease. Vagally mediated bradycardia, but not bradycardia due to cardiac factors, is abolished by atropine treatment. After the initial heart rate is measured, 40 mg of atropine sulfate (as a 1% solution) is injected SC, and the heart rate is measured again 15 minutes later. An increase of 16% or more strongly suggests vagally mediated bradycardia.
Absence of bradycardia, however, does not rule out vagal indigestion, and bradycardia that is abolished by atropine does not prove vagal nerve damage as the cause of indigestion. All cases of vagally mediated bradycardia are affected by atropine, although usually not as strongly as is bradycardia that results from a vagal nerve lesion.
The rumen chloride concentration and the concentrations of serum chloride, total protein, fibrinogen, urea, and potassium are measured in cattle suspected of having vagal indigestion. The results of the glutaraldehyde test and measurements of total protein and fibrinogen concentrations can aid in assessment of the severity of potential inflammatory lesions.
Diagnostic Testing
Ultrasonographic examination is aimed at detecting adhesions and abscesses near the reticulum, liver, omasum, and abomasum that could account for the vagal indigestion;, it determines the frequency of reticular contractions. In a study of 133 cows with vagal indigestion, 58 (44%) had 5–12 (normal is 3–4) reticular contractions every 3 minutes.
Ultrasonography enables the differentiation of distal functional stenosis and ileus of the duodenum or proximal jejunum. The duodenum is greatly dilated in cattle with the latter conditions but not in those with distal functional stenosis.
Radiography aids in the detection or ruling out of reticular ferrometallic foreign bodies as the cause of vagal indigestion, and sometimes foreign material is observed obstructing the reticulo-omasal orifice.
Finally, exploratory laparotomy and rumenotomy may aid in the diagnosis. A finding typical of proximal functional stenosis is massive dilatation and overload of the ruminoreticulum with frothy, nonstratified ingesta and a relatively small and empty omasum and abomasum. The reticulo-omasal orifice is dilated and fails to contract in response to manual stimulation. Cattle with distal functional stenosis have marked dilatation of the abomasum, omasum, and rumen.
Differential Diagnosis
Differential diagnoses for chronic indigestion include ileus of the duodenum or jejunum, frothy ruminal bloat, abomasal impaction, and abomasal ulcer. In a study, vagal indigestion was the principle clinical sign in 26 of 94 (28%) cows with type Ic abomasal ulcer. It is likely that pain associated with the ulcer was the reason for the functional stenosis.
Treatment and Prognosis of Chronic Indigestion Syndrome in Ruminants
Varied treatment, depending on the suspected etiology
The prognosis is unfavorable and treatment is not advised when clinical, ultrasonographic, and radiographic examinations fail to identify a cause of vagal indigestion. The same is true for cattle with positive results of the atropine test and for cattle that develop vagal indigestion within a few days after surgical treatment of RDA or abomasal volvulus. Treatment is indicated in cattle with mechanical obstruction of the reticulo-omasal orifice by materials such as a piece of rope or placenta, with traumatic reticuloperitonitis, with abscesses involving the reticulum and liver, with bronchopneumonia, and in advanced gestation.


Photographs of a 2.5-year-old Piedmontese cow with chronic indigestion attributable to advanced gestation (9 months) before (A) and after (B) calving. A—Note the severe abdominal distention. B—Abdominal distention resolved within a few days after calving, by which time the cow's health status had returned to normal.
Courtesy of Dr. Ueli Braun.

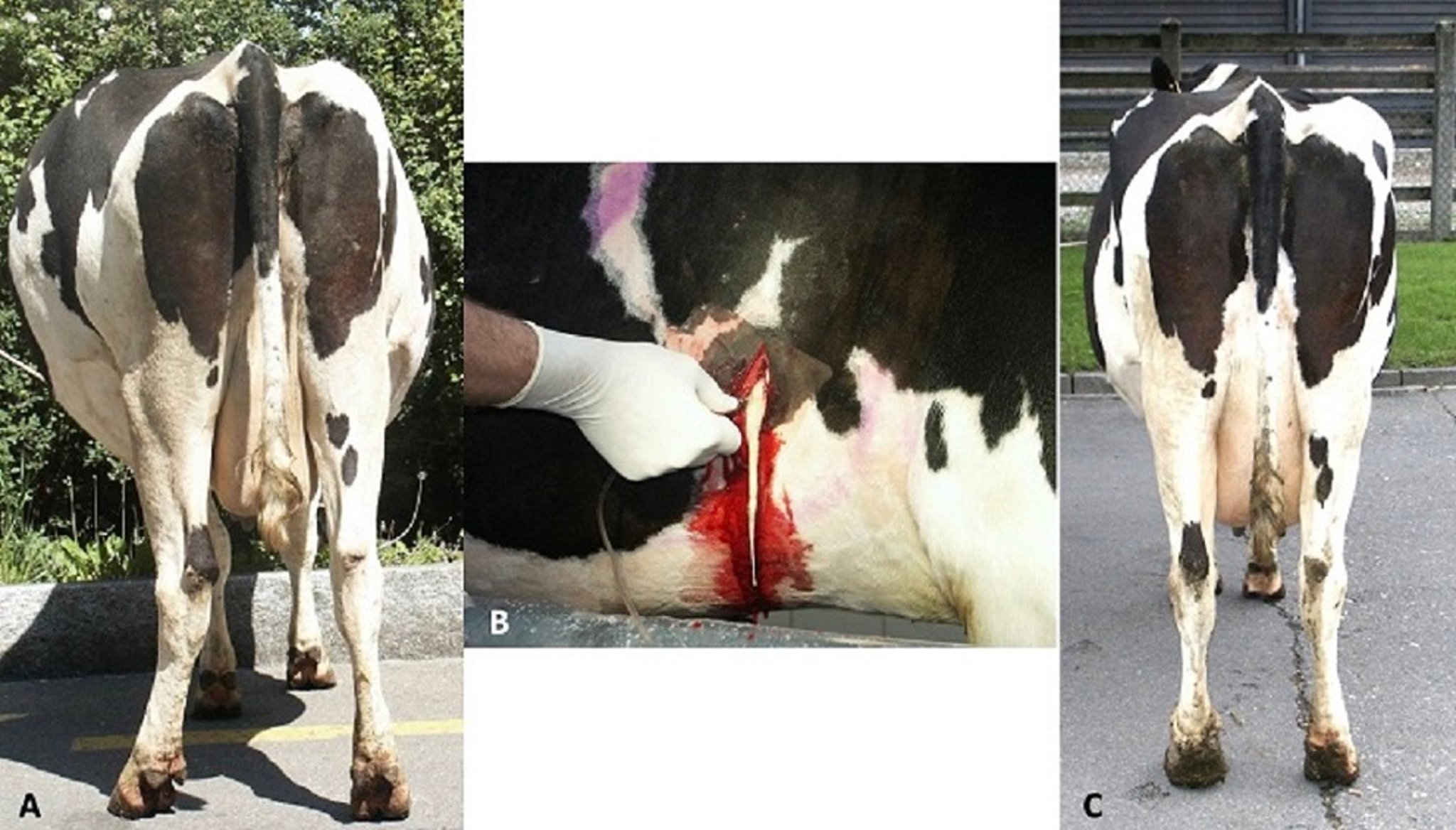
Photographs of a 6-year-old, 7.5-month-pregnant Holstein cow with chronic indigestion attributable to an abscess involving the reticulum and liver. A—The cow had severe abdominal distention with a papple-shaped contour as viewed from behind. B—The abscess, which was 30 cm in diameter, was lanced and drained in the 7th intercostal space on the right side under ultrasonographic guidance. C—The abdominal contour had normalized 10 days after drainage of the abscess.
Courtesy of Dr. Ueli Braun.
The choice of treatment for chronic indigestion depends on the suspected etiology. When the cause of ruminal tympany (most often occurring in calves and young cattle) is bronchopneumonia with a lesion or compression of the vagal nerve due to mediastinal lymph nodes, administration of antimicrobials and NSAIDs can be attempted. In cows in late gestation carrying a viable fetus, induction of parturition may be indicated, which would ideally lead to emptying of the ruminoreticulum and abomasum and a decrease in the rumen chloride concentration.
Cattle with vagal indigestion due to traumatic reticuloperitonitis are treated with antimicrobials and a rumen magnet, or the foreign body is removed surgically. Abscesses involving the reticulum and liver are lanced and drained from within the reticulum or transcutaneously under ultrasonographic guidance.
Foreign materials such as a piece of rope or placenta are removed during rumenotomy. Cattle with ruminal tympany because of failure of eructation are treated with a temporary or permanent rumen fistula. Elective left-flank laparotomy in cattle with proximal functional stenosis is indicated only when ultrasonography and radiography are not available; in most cases, emptying the rumen during rumenotomy without addressing the cause of the disorder provides only transient improvement. Supportive IV fluid therapy, possibly combined with rumen transfaunation, is recommended in all cases.
Prevention of Vagal Indigestion Syndrome in Ruminants
The most common cause of vagal indigestion syndrome is traumatic reticuloperitonitis, which causes adhesions and abscesses that interfere with both reticular motility and the appropriate stratification of feed particles for passage through the abomasum. Therefore, prevention of traumatic reticuloperitonitis is important for preventing vagal indigestion syndrome. Good management practices may prevent some cases of vagal indigestion associated with chronic pneumonia. Early diagnosis of abomasal volvulus, with same-day surgical correction, may prevent some cases.
Key Points
Chronic indigestion (or vagal indigestion) refers to functional or mechanical disturbances of ruminant stomach that impair gastrointestinal transit.
Clinical signs include abdominal and ruminal distension as well as poor appetite, weight loss, dehydration, reduced fecal output, and bradycardia.
Treatment depends on the underlying cause.
For More Information
Braun U, Rauch S, Hässig M. Ultrasonographic evaluation of reticular motility in 144 cattle with vagal indigestion. Vet Rec 2009;164:11-13.
Braun U, Gerspach C, Reif C, et al. Clinical, laboratory and ultrasonographic findings in 94 cows with type-1 abomasal ulcer. Schweiz Arch Tierheilkd 2020;162(4):235-244.
Constable PD, Hinchcliff KW, Done SH, et al. Vagus indigestion. In: Veterinary Medicine. A Textbook of the Diseases of Cattle, Horses, Sheep, Pigs, and Goats. Elsevier; 2017:490-496.
Dirksen G. Funktionelle Stenosen zwischen Netz- und Blättermagen ("Hoflund-Syndrom"). In: Dirksen G, Gründer HD, Stöber M, eds. Innere Medizin und Chirurgie des Rindes. Parey Buchverlag; 2006:415-420.
Sattler N, Fecteau G, Hélie P, et al. Etiology, forms, and prognosis of gastrointestinal dysfunction resembling vagal indigestion occurring after surgical correction of right abomasal displacement. Can Vet J 2000;41:777-785.





