

Ascarid-Associated Colic in Horses
Exposure to Parascaris spp is common worldwide, but disease is exceedingly rare. Two ascarid species infect horses: Parascaris equorum and Parascaris univalens. Little is known about the biological differences between the two species; however, P univalens is believed to be common around the world, whereas P equorum is extremely rare.
Ascarid eggs are regarded as environmentally durable and remain infectious for several years. However, survival depends on temperature; eggs do not tolerate temperatures > 40°C for more than a few days. Eggs are likely to remain viable through the winter in colder climates and be infective the following foaling season after they have embryonated and contain infective larvae.
Once ingested by a horse, ascarid eggs hatch, and L3 larvae begin hepatotracheal migration, arriving in the lungs approximately 1 week after infection. There they penetrate the alveoli and bronchioles, where they remain for approximately 2 weeks before they are coughed up into the pharynx and swallowed to return to the small intestine as L4 larvae.
The first intestinal stages of ascarids appear 3–4 weeks after infection. After approximately 2 more months, the parasites become adults (see ), and they begin shedding eggs 90–110 days after infection.


Ascarid worm burdens are highest when foals are approximately 5 months old, after which a mounting immune response begins clearing the infection, regardless of anthelmintic treatment. Weanlings and yearlings can sometimes become reinfected to a lesser extent, but most ascarid burdens are eliminated before horses reach 1 year old.
Equine ascarid infections can lead to small intestinal impactions. The median age of foals with reported ascarid small intestinal impactions is 5 months, which coincides with the worm burden peak. However, impactions have been reported in yearlings, young adults, and fully mature horses too.
Clinical Findings
Acute parascarosis (disease caused by the parasite) can manifest as impaction in young horses and requires emergency treatment. The typical case of ascarid impaction occurs in a 5-month-old foal that has been recently dewormed with an effective anthelmintic; sometimes, however, the foal will not have been dewormed.
Clinical signs of ascarid-associated colic include the following:
elevated heart rate
dehydration
hyper- or hypoperistalsis
positive gastric reflux
hyperemic mucous membranes
clear signs of pain and limited response to analgesics
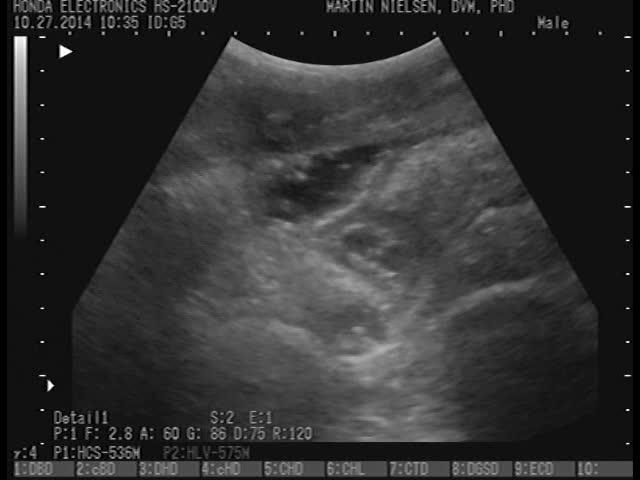
Clinical laboratory findings are typically unremarkable. However, transabdominal ultrasonography can reveal dilated small intestinal loops with hyperechoic worms clearly visible (see ).
The pulmonary stages of Parascaris spp infection have led to bronchitis or bronchopneumonia in experimentally inoculated foals. However, respiratory signs have not been reported as clinically important in naturally infected horses.
Diagnosis
Fecal egg counts
Transabdominal ultrasonographic examination
Ascarid eggs in a fecal sample confirm the presence of sexually mature female parasites, but their presence does not correlate with risk of impaction, because most 5-month-old foals are likely to be ascarid-positive. However, diagnosis of ascarid infection can be confirmed by ultrasonographic visualization and semiquantitation of worms within dilated small intestinal loops (see ).
Treatment
Surgery for acute cases
Benzimidazole anthelmintics
Supportive care
In acute cases of ascarid-associated colic in horses, treatment should be directed at resolving small intestinal impaction. Surgical treatment can include enterotomy and removal of as many worms as possible, or it can be a less invasive procedure to milk or massage parasites into the cecum.
A more conservative medical approach can be taken in cases presenting with controllable signs of pain and without gastric reflux. Mineral oil can be administered along with spasmolytic medication and fluid therapy. A full labeled dose of a benzimidazole should be administered and gastric reflux checked every 3 hours for the initial 24–48 hours or until the patient is stabilized.
Treating ascarid-associated colic in horses with an anthelmintic can exacerbate intestinal impaction, so this approach should be chosen only in cases with manageable pain and without gastric reflux. Progression can be monitored with frequent ultrasonographic examination.
Pearls & Pitfalls
|
Complications of ascarid-associated colic include intussusception, volvulus, or intestinal rupture.
In addition, the following supportive measures can be implemented, if appropriate:
fluid therapy
pain medication
correction of acidosis or alkalosis
anti-inflammatories
antimicrobials
The current recommendation is to include an anthelmintic as part of the treatment plan.
Benzimidazoles are generally recommended not only because of the low resistance rate reported in equine ascarids, but also because of their nonparalytic mode of action in killing worms slowly over 2–3 days.
Given the high rate of resistance to macrocyclic lactones that ascarids are reported to have worldwide, these medications are unlikely to work well against these parasites.
Pyrantel products can be effective but should be used with caution because, theoretically, their paralytic mode of action could lead to intestinal impaction.
If anthelmintic treatment is chosen, dead worms can be recovered via nasogastric tube or left to pass in feces.
Prevention
To minimize the risk of disease caused by ascarids in horses, current recommendations include fecal diagnostic testing, routine monitoring of anthelmintic efficacy, and a combination of strategic and targeted anthelmintic treatments. For ascarids, it is generally recommended to target Parascaris spp twice before weaning, with treatments administered when foals are approximately 2 months old and 5 months old.
Benzimidazoles at the labeled dose are the anthelmintic of choice to prevent ascarid infection in foals. Fecal egg counts determined before and after the 5-month treatment can be used to 1) determine the relative presence of strongyles versus ascarids, and 2) evaluate the treatment efficacy against these parasites and determine the need to target strongyle parasites separately.
Zoonotic Risk
There is no zoonotic risk of ascarid infection in horses.
Strongylus vulgaris–Associated Disease in Horses
The equine bloodworm Strongylus vulgaris is regarded as the most pathogenic equine GI helminth. Historically, the prevalence of S vulgaris was reported to be 80–100%; however, decades of routine deworming have substantially decreased this prevalence in most countries.
S vulgaris belongs to the group of large strongyles (the subfamily Strongylinae in the family Strongylidae). It is one of three Strongylus spp that infect horses. The other two—Strongylus edentatus and Strongylus equinus—have not been associated with distinct diseases and are not covered here.
S vulgaris has not yet developed resistance to any anthelmintics, which is probably the main reason this parasite has become rare in managed horses. S vulgaris can occur in equine operations managed with few or no anthelmintics, and it has been documented as reemerging in countries such as Denmark and Sweden, where anthelmintic use is restricted by prescription-only legislation.
Pearls & Pitfalls
|
As part of the typical life cycle of S vulgaris, ingested third-stage larvae (L3) migrate subendothelially in intestinal arterioles toward the root of the cranial mesenteric and celiac arteries. There they molt to the fourth stage (L4) and enter the arterial lumen, where they molt to the L5 stage. Later they are carried down the circulatory tree to form abscesses (approximately 1 cm in diameter) in the walls of the cecum, ventral colon, and dorsal colon. These abscesses eventually rupture, releasing the larvae into the intestinal lumen.
Most S vulgaris adults are found in the cecum; occasionally, however, a few are located in the ventral colon. The complete life cycle takes approximately 6 months, with approximately 4 months spent in the mesenteric arteries.
In some temperate climates, S vulgaris occurrence and abundance are seasonal, with horses acquiring infections during the grazing season and the migratory phase occurring during winter. As a result, egg-shedding adults are more abundant in spring as these parasites complete their extraintestinal migration.
Clinical Findings
Infection with S vulgaris invariably causes chronic active verminous mesenteric endarteritis (see ); however, this lesion has not been associated with distinct clinical signs. Similarly, clinical signs have not been linked to the formation and subsequent rupture of intestinal abscesses as larvae return to the intestinal lumen. Although S vulgaris adults can attach to intestinal walls and have been reported to ingest blood, they are not described as a primary cause of clinically important anemia in horses.


Chronic active verminous endarteritis in a horse, caused by migrating larvae of Strongylus vulgaris. This necropsy image of an opened cranial mesenteric artery demonstrates the typical lesions: thickened and fibrotic arterial wall, thrombus formation, and the presence of several larvae within the vessel lumen.
Courtesy of Dr. Martin K. Nielsen.
In contrast to the subclinical verminous endarteritis described above, S vulgaris infection can also lead to clinically important peritonitis from thromboemboli that cause nonstrangulating intestinal infarction. Infarction occurs after parasitic migration through intestinal arteries results in arterial wall damage, thrombus formation, and, ultimately, detachment of emboli from the thrombus that flow downstream and occlude small arteries and arterioles. Clinical signs include fever, malaise, variable extents of colic, and sometimes a mass palpable on rectal examination. Also see Thrombosis, Embolism, and Aneurysm in Animals.
Clinical laboratory findings typically include the following:
increased serum amyloid A and fibrinogen concentrations
decreased plasma iron concentration
leukopenia
increased lactate concentrations in plasma and peritoneal fluid
Abdominocentesis reveals fulminant peritonitis with high numbers of white blood cells and increased protein and lactate content.
Diagnosis
Clinical evaluation
Abdominocentesis
Exploratory laparotomy
Coproculture
Clinical signs associated with S vulgaris infection in horses are nonspecific. Abdominocentesis is required to diagnose peritonitis; however, it does not typically identify the causative agent. Where S vulgaris is endemic, patients presenting with peritonitis should be evaluated for nonstrangulating intestinal infarction, which can be definitively diagnosed only by exploratory laparotomy.
Fecal flotation and egg counts have no value for the diagnosis of S vulgaris infection. These tests do not differentiate between various strongyle species. The presence of adult intestinal stages can be more specifically determined with coproculture (fecal culture to detect GI tract bacterial infection) or PCR assay; however, this determination has limited value because the disease is caused by migratory larvae, not by adult parasites.
Pearls & Pitfalls
|
Treatment
Exploratory laparotomy with possible intestinal resection
When intestinal infarction has occurred, medical treatment of S vulgaris–associated disease is generally not successful. Exploratory laparotomy reveals the extent of intestinal damage and indicates whether surgical correction is feasible. The prognosis for patients eligible for immediate corrective surgery is fair to good. In comparison, the prognosis is guarded if surgery is attempted > 24 hours after the onset of clinical signs.
Standard postsurgical care includes the following:
fluid therapy
anti-inflammatories
antimicrobials
There is little or no value in administering anthelmintic medications in the acute phase of a nonstrangulating intestinal infarction in horses. However, deworming with a larvicidal anthelmintic is recommended after the patient is stabilized and peritonitis has resolved.
Anthelmintic options are ivermectin (0.2 mg/kg, PO, once), moxidectin (0.4 mg/kg, PO, once) or fenbendazole (10 mg/kg, PO, every 24 hours for 5 days). The migratory L5 stage may not be fully susceptible to anthelmintic treatment.
Prevention
Current S vulgaris control recommendations include a foundation of anthelmintic treatments administered to all horses, with the specific goal of decreasing the numbers of this parasite. In most locations, control measures should consist of one or two strategically administered yearly treatments with an effective anthelmintic.
Zoonotic Risk
There is no zoonotic risk of S vulgaris–associated disease in horses.
Larval Cyathostominosis in Horses
Cyathostomins are small strongyles that infect all grazing horses to some extent. The cyathostomin parasite subfamily comprises 50 species within 14 different genera. Forty of these species infect horses, and it is common to find coinfections with 10–20 different species in a single horse.
Clinically normal horses can harbor cyathostomin burdens ranging from a few thousand to more than a million worms. In some parasitized horses, however, acute larval cyathostominosis occurs when encysted larvae emerge, en masse, from large intestinal walls. Very little is known about the biological and pathogenic differences between cyathostomin species because of a lack of antemortem diagnostic tools to differentiate them. For this reason, cyathostomins are discussed as a biologically uniform group with regard to pathogenicity and anthelmintic resistance.
In the typical cyathostomin life cycle, ingested third-stage larvae (L3) migrate into the cecal and colonic walls, where they encyst and go through the early third (EL3), late third (LL3), and mucosal fourth (ML4) larval stages (see ). The ML4s then excyst and migrate back into the intestinal lumen as luminal L4s (LL4s) before reaching the final and sexually mature stage (L5).


Photomicrograph showing the mucosal membrane of the ventral colon from a clinically normal horse infected with cyathostomin parasites. Several encysted larvae are visible. Scale bar = 1 cm.
Courtesy of Dr. Martin K. Nielsen.
The EL3 cyathostomin larvae undergo variable amounts of arrested development (hypobiosis) for durations ranging from a few weeks or months to several years. In climates with well-defined grazing seasons, the relative proportion of arrested EL3s can follow a seasonal pattern: EL3s accumulate throughout the grazing season, reaching peak numbers in autumn and winter. As a result, horses (especially those < 5 years old) can harbor hundreds of thousands of encysted larvae.
Larval cyathostominosis occurs when many encysted larvae synchronously emerge from cysts within intestinal walls. Each emerging larva induces an inflammatory reaction, and high numbers can lead to a generalized typhlocolitis that affects primarily the cecum and ventral colon.
Despite the ubiquity of cyathostomin parasites and the accumulation of encysted larvae, larval cyathostominosis is rarely observed worldwide. Most reports of cases have come from countries with northern, temperate climates, and the condition appears to be extremely rare in the US.
Clinical Findings
Typically, acute larval cyathostominosis affects young horses (1–4 years old, rarely foals); however, this condition can occur in mature horses as well. The affected horse has often been recently dewormed with an effective nonlarvicidal anthelmintic. Clinical signs include the following:
sudden onset of profuse watery diarrhea
severe dehydration
varying extents of circulatory shock
edema of the sternal region, prepuce, and distal limbs
possible colic signs
weight loss
elevated, normal, or decreased body temperature
Clinical laboratory findings typically include the following:
neutrophilic leukocytosis
hypoproteinemia and hypoalbuminemia
increased acute-phase protein concentrations (eg, amyloid A, fibrinogen)
lactic acidosis and metabolic acidosis
Diagnosis
Clinical evaluation
Clinical laboratory findings
The clinical signs of cyathostominosis in horses are nonspecific; however, diarrhea is usually present. Typical clinical laboratory findings include hypoalbuminemia and neutrophilic leukocytosis.
No diagnostic tests have been validated for larval cyathostominosis in horses. Fecal flotation and egg counts are not useful, because the condition is caused by larval stages emerging from intestinal walls and not by egg-producing adults. Similarly, both cyathostomin larvae and adult worms can sometimes be observed on a rectal sleeve or in fecal samples; however, this observation only documents the presence of parasites and does not indicate pathology.
Diagnosis of cyathostominosis is based on clinical signs, clinical laboratory findings, and anthelmintic treatment history, as well as on exclusion of differential diagnoses, as follows:
Fecal cultures and PCR testing for salmonellosis, as well as clostridial toxin assays and sampling for Neorickettsia risticii (the cause of Potomac horse fever), are relevant in any case of peracute colitis in North America.
Equine proliferative enteropathy caused by Lawsonia intracellularis is a differential diagnosis with a very similar presentation, and testing for L intracellularis is indicated.
Ultrasonography often reveals markedly edematous cecal or colonic walls, along with fluid in the lumen.
Chronic cases of cyathostominosis can be accompanied by weight loss and edema formation due to severe enteric protein losses.
Treatment
Supportive care
Anti-inflammatories
As with all cases of equine colitis, multifaceted intensive medical treatment—including fluid therapy, electrolyte correction, anti-inflammatories, and, in some cases, antimicrobials—is indicated.
Acute larval cyathostominosis is a serious condition, with a mortality rate of approximately 50%.
The current recommendation for treating acute larval cyathostominosis in horses is to include a larvicidal anthelmintic. However, neither of the two currently labeled anthelmintics are likely to be completely effective:
A single oral dose of moxidectin (0.4 mg/kg) has been documented to decrease the number of later larval stages (LL3 and mucosal L4) by approximately 60–80%; however, this effect may last only approximately 5 weeks in horses kept on pasture.
A 5-day regimen of oral fenbendazole (10 mg/kg in North America, 7.5 mg/kg in Europe) is claimed on the label to be effective against all larval stages; however, studies have documented a 50–70% efficacy (1), which is clearly lower than historical efficacy values.
Prevention
Current parasite control recommendations are designed to decrease risk of larval cyathostominosis through fecal diagnostic testing, routine monitoring of anthelmintic efficacy, and a combination of strategic and targeted treatments. Coupled with good pasture management and regulation of stocking density, this approach should decrease parasite contamination of pastures and decrease infection pressure.
Anthelminthic resistance of cyathostomins is increasingly common. Equine cyathostomins have been widely reported as resistant to pyrimidine and benzimidazole anthelmintics. Several reports have documented resistance to macrocyclic lactones as well.
Zoonotic Risk
There is no zoonotic risk of larval cyathostominosis in horses.
Tapeworm-Associated Colic in Horses
Tapeworm infection is common in grazing horses and can cause ileal colic. Three tapeworm species infect horses:
Anoplocephaloides mamillana (formerly Paranoplocephala mamillana)
Anoplocephala magna
Anoplocephala perfoliata
The first two of these species have become rare in managed horses. The only species with documented clinical impact is A perfoliata, which commonly occurs in grazing horses worldwide; however, it tends to be rare or absent in arid climates.
Free-living and commonly occurring oribatid mites, accidentally ingested by horses while grazing, act as intermediate hosts for A perfoliata. The mites carry the infective stage of the parasite (the cysticercoid), which is digested free of the mite’s tissue in the horse's intestinal tract and forms a scolex.
A perfoliata scolices attach to the cecal wall and tend to cluster around the ileocecal valve (see ). With large parasite burdens, worms can be found in the ileum as well.


Anoplocephala perfoliata adults attached to the cecal wall.
Courtesy of Dr. Martin K. Nielsen.
As they mature, A perfoliata worms form proglottids (tapeworm segments), which contain eggs and are released into intestinal contents. The proglottids subsequently disintegrate, releasing eggs into the intestinal lumen.
Tapeworm-associated colic can occur when large numbers of A perfoliata attach to cecal and ileal walls. Such infection can lead to mechanical obstruction, as well as to mucosal damage ranging from mild hyperemia to multiple confluent necrotic ulcers at attachment sites. These ulcers are speculated to cause intestinal hyperperistalsis and subsequent intestinal spasms, ileal impactions, and ileocecal intussusceptions.
In countries with distinct seasonality and grazing seasons, the presence of mature tapeworms in the intestines is often lowest during summer and highest in winter and early spring, reflecting fluctuations in pasture infectivity.
Clinical Findings
Tapeworm-associated colic can occur in horses of any age and can present with a variety of clinical signs, depending on the pathology in affected organs. In cases of ileal impactions or ileocecal intussusceptions, clinical signs can include elevated heart rate, abdominal pain, and sometimes a firm intestinal mass palpable rectally.
Clinical laboratory findings are generally unremarkable but can include leukocytosis and neutrophilia.
Diagnosis
Clinical evaluation
Fecal egg counts
Serological examination
Rectal palpation and/or ultrasonographic examination can suggest ileal impaction or intussusception. Detection of tapeworm eggs (see A perfoliata ) on fecal examination confirms the presence of adult tapeworms; however, it does not document a causative relationship. Serum and salivary antibody ELISAs are available in some countries; however, they only reflect parasite exposure and do not necessarily indicate a causative relationship.


Photomicrograph showing an Anoplocephala perfoliata egg, distinguished by the pyriform apparatus containing the hexacanth embryo. Scale bar = 20 mcm.
Courtesy of Dr. Martin K. Nielsen.
Although definitively identifying tapeworms as the cause of colic has limited implications for managing acute cases, it is valuable for subsequently advising clients about future herd management. Standard fecal tests lack diagnostic sensitivity; however, modified techniques with better sensitivity exist.
The reliability of currently available equine tapeworm diagnostic methods has been well investigated, and standard egg-counting techniques (eg, the McMaster technique) have been shown to have a diagnostic sensitivity of < 10%, making them practically useless for this purpose. However, some modified egg-counting techniques have a sensitivity of approximately 60% for detecting any tapeworm burden and 90% for detecting the more clinically relevant burden of > 20 worms. These modified techniques require the processing of larger amounts of fecal matter, as well as centrifugation to concentrate and float eggs.
Repeated episodes of spasmodic colic in horses are sometimes assumed to be due to tapeworm infection. Although tapeworms cannot be ruled out, other etiologies should be considered. A positive fecal test can help support the tentative tapeworm diagnosis.
Treatment
Pyrantel pamoate, double dose
Praziquantel
Cases of ileal impaction or ileocecal intussusception require surgery and standard perioperative supportive care.
The current recommendation is to consider anticestodal treatment only after colic has resolved and the patient has stabilized. A double dose of pyrantel pamoate (pyrantel embonate; 13.2 mg of pyrantel base/kg, PO, once) or products containing praziquantel (1.0–2.5 mg of praziquantel/kg, PO, once) are generally considered effective options. However, evidence of treatment failure has been reported for both anthelmintics.
Prevention
Current parasite control recommendations are designed to minimize the risk of parasitic disease. Serum or saliva antibody testing can help determine the tapeworm infection pressure within an equine operation. Results of such testing can guide decisions about whether to include anticestodal treatments in the control strategy.
On most farms, current recommendations are to treat for tapeworms at least once a year, in autumn. Evidence of high infection pressure or cases of tapeworm-associated colic on a farm can justify more frequent treatments. Overall, the aim is to decrease parasite contamination of pastures and thereby decrease infection pressure.
Zoonotic Risk
There is no zoonotic risk of tapeworm infection in horses.
Key Points
Parascaris spp parasites are ubiquitous in foals worldwide; however, verminous small intestinal impactions are extremely rare.
Strongylus vulgaris infection is rare in most managed equine populations; however, it can reemerge with limited or restricted anthelmintic use.
Cyathostomins are ubiquitous, but larval cyathostominosis is extremely rare.
Anoplocephala perfoliata is very common and can cause ileocecal colic.
Cyathostomins, ascarids, and A perfoliata have developed resistance to widely used anthelmintics.
For More Information
American Association of Equine Practitioners (AAEP): Internal Parasite Control Guidelines
Also see pet owner content regarding GI parasites of horses.
References
Nielsen MK. Anthelmintic resistance in equine nematodes: Current status and emerging trends. Int J Parasitol Drugs Drug Resist. 2022;20:76-88. doi:10.1016/j.ijpddr.2022.10.005





