

Managing pet birds in the clinical setting can be challenging. Because birds have the ability to “mask” clinical signs of illness until late in the disease process, they often are not presented until much sicker than owners realize. This also means that birds are riskier patients to evaluate. Birds have a much higher metabolism than mammals, and oxygen deprivation can occur during restraint, treatment, or diagnostic sampling. Owners should be informed of the risks of handling and sampling and the need for a step-by-step approach through the physical examination and diagnostic testing. Placing severely debilitated birds in a warm oxygen incubator or cage while obtaining the history and before conducting the physical examination may be warranted. Before restraining the bird, it is important to be prepared with all needed items for examination, sample collection, and treatments.
Items needed for examination and sample collection include:
gram scale
light source
oral speculum
stethoscope
syringe and needle for venipuncture
blood tubes/slides
subcutaneous fluids if needed
If a bird is extremely stressed, in pain, or not used to handling, sedation before examination and diagnostic testing may be warranted.
Taking a Medical History of Pet Birds


Blue and gold macaw.
Courtesy of Dr. Sharman Hoppes.


Scarlet macaw.
Courtesy of the Schubot Exotic Bird Health Center.
Having the owners bring a pet bird in its own cage for examination is desirable but often impractical. Alternatively, owners can be asked to bring photos or videos of the cage set-up, as well as recent papers from the cage floor so the droppings can be examined. The history should include:
source of the bird and whether hand raised or parent raised
exposure to other birds or pets
length of ownership and history of previous owners
time spent outside of cage and if supervised
interactions with humans or other pets
exposure to outdoors
cage brand, size, and bar spacing
type of substrate and how often changed
frequency of cleaning of cage, food, and water bowls
location of cage in the home
temperature and humidity of home
diet offered and foods actually eaten
recent changes in diet or appetite
presenting problem
previous health issues




Green-winged macaw.
Courtesy of the Schubot Exotic Bird Health Center.
The length of time a bird has been in the household is usually inversely proportional to the probability that illness will be caused by a primary infectious disease. Newly acquired birds or those exposed to other birds outside the household via bird shows or pet store visits are most likely to be affected by infectious diseases. Chronic malnutrition and secondary infections are more common in birds without recent exposure to potentially infectious birds. Malnutrition is a major cause of subclinical disease in birds, which predisposes them to secondary infections.


Sulfur-crested cockatoo.
Courtesy of Dr. Sharman Hoppes.


Cockatiels.
Courtesy of the Schubot Exotic Bird Health Center.


Quaker parrot.
Courtesy of Dr. Sharman Hoppes.
Clinical signs of illness can be difficult to detect in birds. However, astute owners may recognize minor behavioral differences in their bird, such as not vocalizing in the morning or decreased interaction with family members. These changes should be considered potential signs of illness. Owners with less experience or less interaction with their birds are less likely to notice early signs.
Feathers can effectively mask even severe emaciation or abdominal distention. Owners may notice other signs of illness, such as changes in droppings or vocalizations, or if the bird is sleeping more. Veterinarians who see avian patients should be able to identify common species of pet birds (cockatoos, Amazon parrots, macaws, conures, etc) and be familiar with normal species-specific behaviors. For example, parrots of Pionus spp often make rapid sniffing noises when stressed that can be mistaken for respiratory distress.
Physical Examination of Pet Birds
The first step in conducting a physical examination of a pet bird is an observational examination:
perform from a non-threatening distance
observe respiratory rate and effort, presence of open-mouth breathing
observe mentation: alert, active, eyes open or closed
observe posture: perching, tail bobbing, wing position, use of one or both legs
The bird should be observed in the cage or carrier before manual restraint. A respiratory rate should be obtained before handling. The normal resting respiratory rate for pet birds varies with size and species, with the rate ranging in smaller birds (< 300 g) from 30−60 breaths/minute and in larger birds (400–1,000 g) from 15–30 breaths/minute. If the bird is showing signs of respiratory distress, it should be placed in a warm, oxygenated incubator before restraint.


Proper restraint for a Quaker parrot.
Courtesy of the Schubot Exotic Bird Health Center.
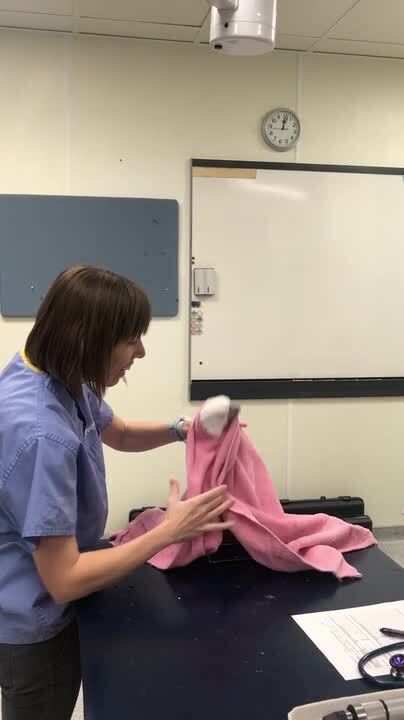
Birds should be restrained in a manner that minimizes stress and does not cause undue fear. If the bird is used to being handled, often a towel can be slowly and gently placed over the bird. If an owner has worked with the bird at home with a towel, the veterinarian may ask the owner to towel the bird and then hand it off for examination or testing. Minimizing restraint time, talking to the bird in a quiet voice, and moving slowly can help reduce stress in many birds. Baby birds or hand-raised cockatoos often can be examined with minimal to no restraint. Many pet birds will step out of the cage or on to a hand and can be gently toweled. Some nervous birds may benefit from sedation for examination and diagnostic testing. Birds that are not handled routinely (breeding or aviary birds) may have to be gently toweled directly from the cage or carrier.
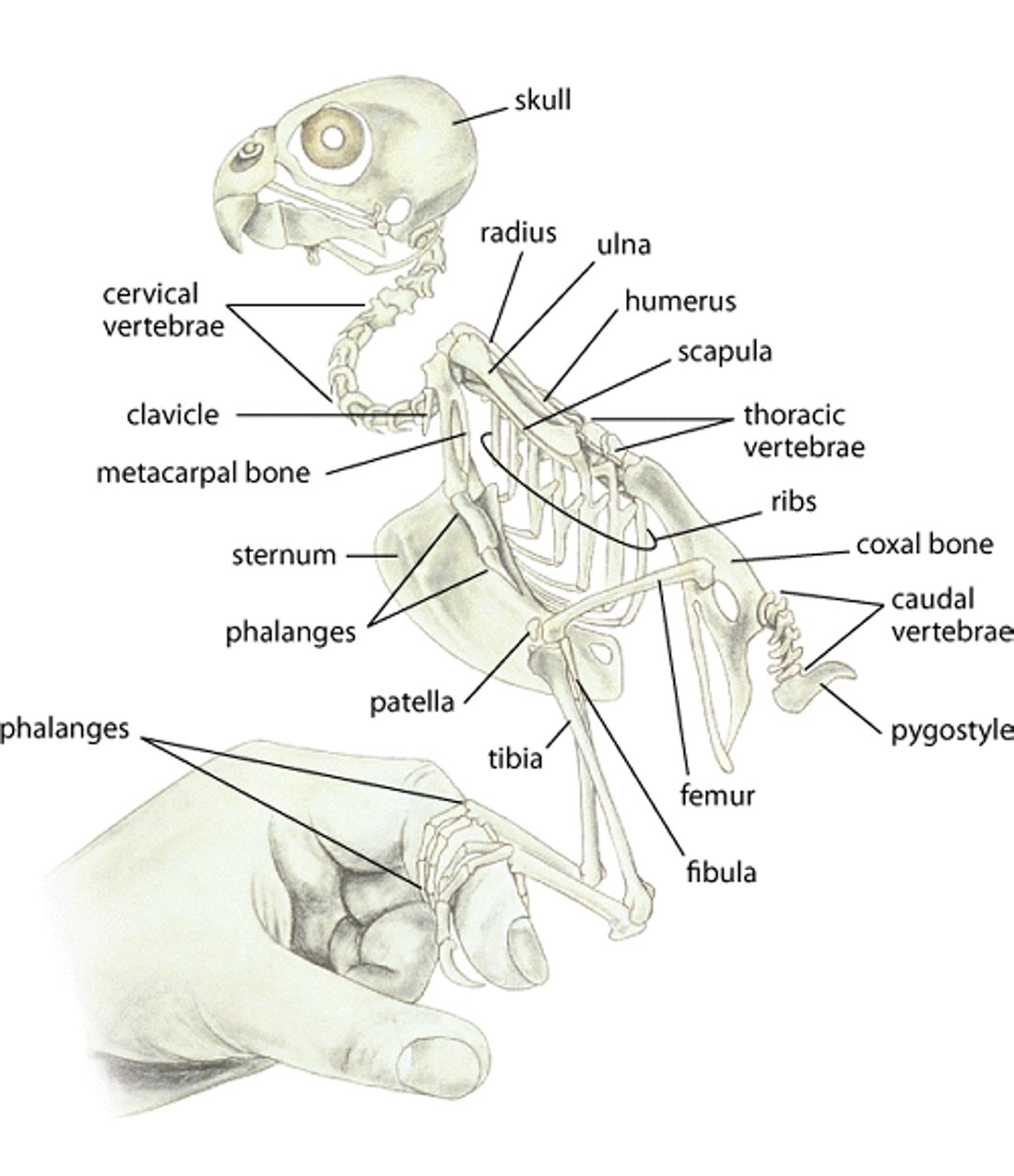
Budgerigar skeleton
Skeleton of a budgerigar. Illustration by Dr. Gheorghe Constantinescu. |

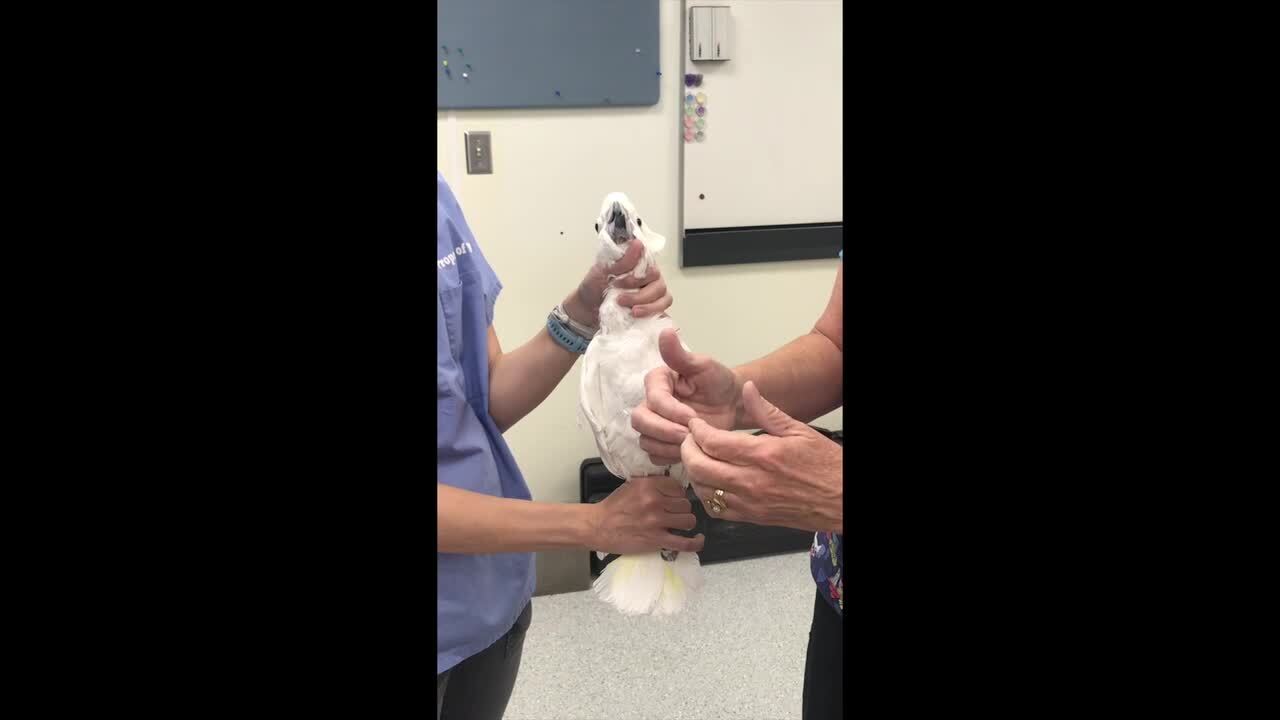
Restraint of psittacine birds involves immobilizing the head, generally with a thumb on one side of the mandible and the index or middle finger on the other. The feet and the distal reminges (primary wing feathers), if not trimmed, are held by the opposite hand in medium to large parrots. This leaves the thorax and abdomen free to expand with respiration. If the primary wing feathers have been trimmed, a towel may be useful to prevent the wings from flapping during restraint. Birds should be observed closely during restraint; all birds can become stressed, and obese birds can overheat, especially when held in a towel. If respirations become increased or labored, or if the bird becomes weak, the bird should be returned to its cage.
As soon as the bird is picked up, the crop should be palpated to determine whether food or fluids are present. If the crop is full, the bird should be monitored for any signs of regurgitation during restraint. Diagnostic procedures may need to be delayed until the crop empties. An accurate weight is critical to monitor health, body condition, and recovery from illness and to determine fluid therapy, nutritional needs, and medication doses.
The ears, eyes, nares, and oral cavity should all be examined and appear clean, with no exudate, masses, or swellings. The choana on the roof of the oral cavity should have intact sharp papilla. Blunted choanal papilla can be a sign of vitamin A deficiency. Exudate around the nares can indicate respiratory or sinus infection, and debris on the feathers of the head or face can indicate vomiting or regurgitation. The condition of the feathers and skin should be noted, including the symmetry and integrity of the beak and nails. Overgrown beak and nails can indicate poor husbandry or nutrition, or liver disease. The integument of the feet should be intact, without excessive wear, callus, or ulceration. Excessive wear of the plantar surface of the feet can indicate inadequate perching or poor nutrition. Excessive wear or callus unilaterally may indicate a problem with the contralateral foot.
Body condition can be determined by palpating the pectoral muscles. A keel scoring system from 1–5 is often used, with 1 as emaciated, 1+ as very thin, and 5 as obese; 3 is an appropriate score for most pet birds. Severely obese birds may deposit fat over the neck, thighs, and abdominal cavity. Wings and legs should extend and flex fully, and grip strength should be symmetrical.

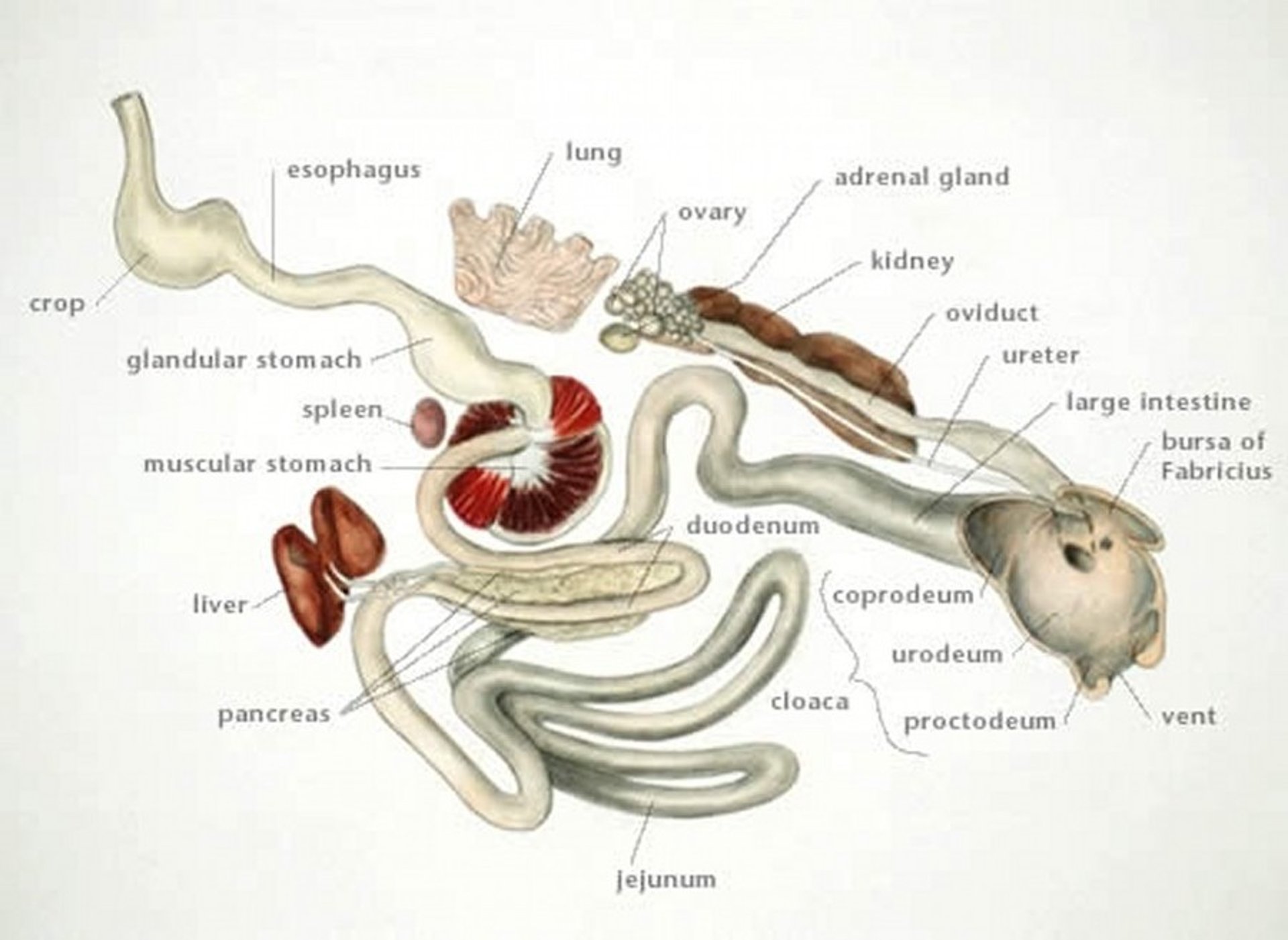
Viscera of a budgerigar.
Illustration by Dr. Gheorghe Constantinescu.
Respiratory rate should be monitored throughout the examination; respirations may increase with hyperthermia, stress, or obesity. Respirations should normalize within 3–4 minutes after the bird has been released. Heart rate is rapid in restrained birds; typically, a large parrot will have a heart rate of >250 beats/minute when restrained. Arrhythmias may occur but can be difficult to categorize because of the rapid heart rate. The cloaca should have sufficient tone to provide tight closure, the skin should be moist, and the feathers around the vent should be clean.
Routine Grooming Procedures of Pet Birds
Wing trimming is frequently requested by owners. Communication with owners about wing trims is vital and should include the degree and purpose of the wing trim. If owners can provide a safe environment for flight, wing trimming may not be recommended. Flight is a natural behavior and provides exercise.

Owners may assume that a wing trim is required at regular intervals. In captivity, however, the frequency at which feathers molt varies based on nutrition, exposure to natural sunlight, photoperiod, and humidity. The fact that a wing trim is a deterrent to flight, but does not guarantee lack of flight, should be emphasized. A bird that can only glide to the ground indoors may be able to fly outdoors on a windy day. If a wing trim is done, only the primary flight feathers should be trimmed; the number of feathers trimmed is based on the weight and flight ability of the individual bird. Heavier birds typically need fewer feathers trimmed, and lighter birds need more.
The basic types of wing trims are:
Removing 4–7 of the distal primary flight feathers from both wings, below the level of the coverts. The number of feathers that must be removed is inversely proportional to the bird’s weight.
Leaving 1–4 distal primary feathers and removing the remainder of the primaries from both wings. This clip has fallen out of favor, but some owners have used it for many years.
Trimming the feathers on only one wing is not recommended.
Excessively aggressive wing trims, especially when performed at the same time as a nail trim, can cause both physical and psychological damage to birds. The sudden lack of stability and lift can cause birds to fall, possibly injuring either the beak or the carina of the keel. This lack of stability can lead to serious behavioral problems, especially in young birds that are learning to fly.
Nail trimming is often requested, frequently for the owner’s comfort and not because of true overgrowth of the nails. Because nail trimming decreases the bird’s stability and increases the chance it will fall from its perch, blunting the needle-like tip while still leaving sufficient nail to allow a stable grip can be a reasonable compromise.
Various types of equipment can be used for nail trims, depending on the size of the bird. Human fingernail trimmers work well to remove the tips of the nails from very small birds. Cat claw trimmers, White’s nail trimmers, and hobby drills with sanding bits are all useful. Sanding tools are also excellent to remove excess keratin that can accumulate on the lateral surfaces of the beak. Beak trimming is sometimes necessary for an overgrown upper or lower beak. Birds with beak deformities often have underlying nutritional deficiencies, disease, or previous trauma. Healthy birds provided adequate environmental abrasive surfaces rarely require beak trims.
In previous decades when parrots were widely imported, open-rolled steel bands were used to identify the location at which they were quarantined. Now most birds are leg banded (using closed bands) as chicks for individual identification. Bands present certain hazards to the bird, but removal also entails some risk if the proper equipment is not available. The open (gap present), rolled, steel quarantine bands are extremely strong and require removal by a full-size bolt cutter with sharp edges. The closed aluminum bands placed on young, captive-raised birds must be stabilized to prevent twisting while being cut. These bands require two cuts to remove; a sharp, properly designed instrument for removal decreases the danger of leg trauma. Full-circle plastic bands can be removed in the same manner.
Microchipping is replacing or augmenting banding as a means of identification. The standard for placement of these chips in psittacine birds is in the left pectoral muscles. Adverse reactions or failures in birds have been infrequent; the intramuscular placement reduces the risk of microchip migration. A standard size microchip can be placed safely in larger parrots with good breast muscle (>150 g). The mini microchip is recommended for smaller birds (< 150 g). The implanter should be directed in a caudal (downward) direction and digital pressure and tissue glue used to seal the implantation site.
Clinical Pathology of Pet Birds
Hematologic testing and plasma biochemical analysis are especially important in birds, because physical examination tends to be less revealing than in other animals. The quantity of blood that can be drawn depends on the weight and health of the bird. Blood collection should be limited to 1% of body weight. Blood is usually collected from the right jugular vein, which is larger than the left. The basilic (wing) vein can also be used but is prone to hematoma formation. In medium to large psittacine birds, seabirds, and poultry, the medial metatarsal vein can be used. Coating a syringe with an anticoagulant before collection may be helpful in smaller species in which sample collection may take longer but can cause artifacts in the blood smear, affecting the differential cell count.

The normal PCV varies between psittacine species. For example, cockatiels normally have a higher PCV than many other species, averaging 50%–55%. Cockatoos (Cacatua spp) often have a PCV in the 40%–45% range.
Anemia can be a result of blood loss or decreased production. Blood loss can occur in cases of trauma or severe organ disease or in idiopathic cases such as conure bleeding syndrome. Response to blood loss anemia may include the presence of immature erythrocytes and anisocytosis along with increased polychromasia. Decreased RBC production can occur with any chronic disease, and the anemia is often non regenerative. Ingestion oftoxins such as lead or oil can result in hemolytic anemia.
Polycythemia is rare in birds and is defined as a PCV >70%. It has been reported in birds with chronic respiratory diseases and in macaws with pulmonary hypersensitivity syndrome, a condition that occurs in macaws housed in poorly ventilated areas with birds that produce large amounts of powder down such as cockatoos, cockatiels, and African grey parrots.
Avian RBCs are nucleated, so traditional methods used to determine WBC counts of mammalian blood are not adequate. Various diluents are available to enable accurate WBC determinations. Estimated WBC counts are less accurate but can be useful when the individual performing the estimate produces blood smears of consistent quality and thickness. Normal total WBC counts vary with species and age. Adult cockatiels often have total WBC counts of 4,000–7,000 × 103/mcL. WBC counts of adult macaws are usually at the high end of the normal avian range (12,000–15,000 × 103/mcL). Stress leukograms are common in parrots after transportation and handling.
A leukocytosis, and the differential or type(s) of WBCs that are increased, can help identify underlying disease and give an indication of the most likely cause. The differential count in birds can be affected by bacterial, fungal, and viral diseases, as well as toxins. The types of avian WBCs are the heterophil, eosinophil, monocyte, and basophil.
Heterophils are equivalent to mammalian neutrophils, with much the same function. Avian heterophils contain lysosomal enzymes and are bactericidal and phagocytic. They are the first cells to respond to any infectious or inflammatory disease process. Instead of forming a liquid purulent material, avian heterophils form an inspissated, caseous material. This caseous material is then walled off by macrophages and fibrous tissue to form a granuloma. Heterophilia can occur during infection or from stress. Heteropenia is often associated with an overwhelming infection or viral disease.
Lymphocytes function in antibody and antigen production and in cellular and humoral immune reactions. Lymphocytosis may occur in chronic infections (chlamydial, fungal, mycobacterial) or with lymphoid neoplasia. In some species (eg, canaries and Amazon parrots), up to 70% of the WBCs are normally lymphocytes. Lymphopenia is often associated with viral diseases (eg, circovirus or polyomavirus) or sepsis.
Monocytosis is often associated with chronic granulomatous diseases such as chlamydial, fungal, or mycobacterial infection. Eosinophilia has been reported with parasitic diseases and has also been associated with delayed hypersensitivity reactions. Basophilia can occur during inflammatory conditions and chronic infection.
Physiologic differences in birds create variations from accepted mammalian normal values for many biochemical measurements. Because of the excretion of uric acid rather than urea as the primary product of protein metabolism, uric acid levels are significantly higher in birds than in mammals, whereas BUN is significantly lower. Uric acid may be increased in severe renal disease or with articular gout. Severe dehydration may increase uric acid levels, but levels return to normal with rehydration. No reliable biochemical indicator is currently available to detect early renal impairment.
Serum or plasma glucose is higher in birds than in mammals, with levels of 250–400 g/dL common, depending on species. Levels that indicate diabetes also vary with species and individuals but often are >700–800 g/dL.
Concentrations of AST and LDH are commonly measured; normal concentrations in birds (AST , 10–400 U/L; LDH, 75–450 U/L) are several times those of mammals. Measurement of creatine kinase (CK) concentration is often performed concurrently to differentiate increased values of AST concentration due to muscle necrosis from those due to hepatic damage. LDH is a short-lived enzyme of limited usefulness in detection of hepatic necrosis. ALT concentrations are very low compared with those in mammals (5–15 U/L); however, increased levels can indicate hepatocellular necrosis.
Birds have low bilirubin reductase concentrations; therefore, total bilirubin concentration is normally very low, and increases with hepatic disease are not consistent (total bilirubin concentration, reference range 0–0.1 mg/dL). Birds do not become icteric with hepatic disease; they excrete biliverdin through their kidneys, resulting in yellow or lime-green urates. Bile acid measurements are useful indicators of hepatic function, with levels < 100 mcmol/L considered normal for most avian species (depending on the laboratory). Establishing reference values for different avian species will enhance the usefulness of bile acid assays.
Calcium and phosphorus values are similar to those found in mammals. These levels may increase up to 3-fold in hens in preparation for egg laying (ie, calcium ~30 mg/dL and phosphorus >10 mg/dL), usually with a relatively normal ratio of these minerals. Total solids as measured via refractometer are significantly lower in birds than in mammals, with levels of 3–5.5 g/dL normal for most species. Total solids can also increase in reproductively active hens.
Cholesterol and triglyceride reference ranges are still being evaluated, but reference values are ~180–250 mg/dL for cholesterol and 51–120 mg/dL for triglycerides. Increased levels of both triglycerides and cholesterol have been reported in birds fed a high-fat diet. High levels can also be seen in reproductively active females and may be a risk factor in birds that develop atherosclerosis. Omega-3 fatty acids added to the diet as well as dietary restriction and conversion to a pelleted diet have been shown to reduce hypertriglyceridemia and hypercholesterolemia.
Hematology and Plasma Biochemistry of the Neonate
Neonates have some important differences from mature birds in their hematologic and biochemical parameters.
Compared with adult birds, neonates have:
lower PCV (20–30%); the normal adult range is present at 10–12 weeks in most species
lower total protein (1–3 mg/dL) and plasma albumin concentrations
higher WBC count (20,000–40,000 cells/mcL is common in neonates); the normal adult range is present at 9–11 weeks of age
lower uric acid levels
higher alkaline phosphatase and CK concentrations
Routine Medical Procedures in Pet Birds
for most medications, subcutaneous injections are as effective as intramuscular injections, without the associated muscle necrosis
fluids should be warmed to 102°–106°F (38.8°–41°C)
sites of subcutaneous administration are the lateral flank, the inguinal web, and the back
intramuscular injections are given into the pectoral muscles in most pet birds
indwelling intravenous catheters can be placed in the jugular, basilic, or medial metatarsal vein
intraosseous catheters are generally placed in the proximal tibiotarsal or distal ulna
Injections can be given by several routes. Subcutaneous injections are used for fluid administration, some vaccinations, and many routine medications such as antimicrobials. Most studies have shown that the subcutaneous route is as effective as intramuscular injections for most medications, without the associated muscle necrosis. To ensure that the medication or fluid being injected is actually deposited subcutaneously, the skin must be clearly visualized; use of alcohol to wet the skin and feathers is recommended to aid in visualization. Insulin syringes (50 U or 0.5 mL) with 27-gauge needles are invaluable for accurate dosing when small quantities must be administered.
Subcutaneous fluids are often used in birds. To maximize their absorption and minimize discomfort, fluids should be warmed to 102°–106°F. Sites of administration are the lateral flank, the inguinal web, and the back. Maintenance fluids are estimated at 50–100 mL/kg/24 hours. In dehydrated birds, half the fluid deficit is given throughout the first 24 hours, and the remaining half is given throughout the next 48 hours.
Intramuscular injections are given into the pectoral muscles in most pet birds; leg muscles are also used in some species, particularly raptors. The muscle fibers of birds are more vascular and tightly packed than those of mammals, making both muscle necrosis and inadvertent intravenous injection more likely.
Intravenous injections are occasionally indicated in birds. Common medications administered intravenously are antimicrobials, amphotericin B, chemotherapeutic drugs, contrast media, and fluids.
Indwelling catheters can be placed in the jugular, basilic, or medial metatarsal veins for constant-rate infusions or intermittent fluid administration. Intraosseous (IO) catheters can also be inserted, generally in the proximal tibiotarsal bone or distal ulna. A standard hypodermic needle may be used (usually 25-gauge for initial entry, followed by a second 22-gauge needle sutured in place), or a spinal needle with stylet may be used for large birds. Without a stylet or second needle, a bone plug may obstruct the needle. The IO or IV catheter is intermittently flushed with warm saline whenever fluids are not being infused. Maintaining an IV catheter in an avian patient can be challenging, and IO catheters are often preferable for longterm fluid therapy. However, fluid therapy via IO catheters can be painful.
Crop (gavage) feeding may be used to meet caloric needs in anorectic birds and is an effective means to provide nutritional support to many birds. Commercial formulas are available and convenient to use. Adequate hydration and normal body temperature (103°–106°F [39°–41°C]) must be established before initiating crop feeding to prevent desiccation of the crop food and GI stasis. Tube feeding formula should be fed at 102–105° F (38.8–40.5°C). In adult birds with crops, generally 30 mL/kg can be administered 3 to 4 times a day. Baby birds have a much more distensible crop and will hold ~10% of their body weight per feeding (100 mL/kg).
Oral medications may be added to the crop feeding or given directly by mouth. The technique of holding the bird so that the medication is administered into the commissure of the mouth and rolls onto the tongue will minimize stress, loss of medication, and the danger of aspiration.
Medicating birds can be quite difficult for owners; wrapping the bird in a towel for administration of medication can be stressful for both the bird and the owner and, in some cases, adversely affect the human-bird bond. Compounding medications to make them more concentrated and palatable can be very helpful when administering oral medications. Mixing the flavored medication with favorite foods, juice, or baby food can also help ensure compliance. Encouraging owners to target-train their birds to accept fluids in a syringe before illness helps facilitate medicating when it becomes necessary.
Medications administered in the water are indicated only in special circumstances such as flocks of small birds or aviary birds not used to handling, or in special cases in which an owner cannot handle a bird. Enrofloxacin and doxycycline in drinking water generally provide adequate blood levels for efficacy. However, lack of accurate dosing, stability of the medication, and palatability make this route undesirable in most cases.
Sedation is sometimes desirable for diagnostic or treatment procedures to reduce stress and minimize fear. Midazolam administered at 0.5–1 mg/kg, IM, or 1–2 mg/kg intranasally (IN) is a safe and effective sedation protocol in most pet birds; flumazenil (0.02–0.1 mg/kg, IM or IN) may be given to reverse the effects. If the bird is thought to be in pain or discomfort, butorphanol (0.5–3 mg/kg, IM or IN, depending on species) may be given alone or with midazolam. Amazon parrots often require the higher dosage (2–3 mg/kg) of butorphanol, whereas raptors require the lower dosage (0.5 mg/kg). Isoflurane or sevoflurane anesthesia delivered by face mask can also be used alone or in conjunction with sedation for more prolonged procedures or painful treatments.
Intubation in birds is relatively easy, because the absence of an epiglottis facilitates visibility of the tracheal opening and arytenoids. Fasting before anesthesia should be of minimal duration; fasts of 4–6 hours are typical. Regardless of the duration of the fast, the crop should be palpated for the presence of food or fluid before anesthesia. Delayed crop emptying is common in clinically ill birds. If anesthesia must be administered to a bird with food or water still in the crop, fluid should be removed by a feeding tube if possible, and the head should be elevated for the duration of anesthesia, regardless of whether the bird is intubated.
Endotracheal tubes should be uncuffed, because the absence of a tracheal ligament increases the risk of tracheal necrosis if a cuff is overinflated. Even an uncuffed tube can cause tracheal damage or necrosis; therefore, after the bird is intubated, head movement should be minimized. A small-animal ventilator can be used for most birds as small as 100 g and can greatly improve ventilation during anesthesia. If a mechanical ventilator is not available, manual intermittent positive-pressure ventilation will increase oxygenation in anesthetized birds. A capnograph, pulse oximeter, and Doppler are also useful for anesthetic monitoring.
The normal body temperature of most psittacines is 103°–106°F (39°–41°C). Birds tend to lose body heat rapidly when anesthetized, and maintaining body temperature during prolonged anesthesia or surgery is crucial for recovery. Birds with feather loss are more at risk of hypothermia. Water warming blankets under the bird or specialty patient-warming products can be used effectively to maintain body temperature. An emergency drug sheet and emergency drugs should be readily available whenever a bird is anesthetized.
Environmental management is very important; severely ill birds benefit greatly from increased environmental temperature and humidity (eg, use of commercial incubators with temperature and humidity controls). Digital thermometers with remote probes can provide accurate monitoring of environmental temperatures. A quiet location, away from the sound of barking dogs and other excessive activity, will decrease stress.
The cage arrangement can be critical for ill birds. If a perch is supplied, the food and water must be elevated so that the bird has ready access without having to climb down from the perch. Often, it is best to remove perches entirely from the cage of an ill bird and place the food and water container on the cage floor so that the bird has easy access and does not expend energy simply trying to maintain a perched position.
Nutrition of Pet Birds
Although avian nutrition has greatly improved in the past decades, nutritional disease is still common in pet birds. The availability of formulated diets and hand-feeding formulas has been pivotal in improving avian nutritional health, but many birds are still fed inadequate diets. The two most common reasons for malnutrition in companion birds are feeding of diets that allow the birds to choose what they want to eat (either mixtures of seeds/nut and pellets or table foods the owner considers healthy) and feeding of pure seed or seed-based diets. Feeding a mixture of pellets and seeds is also common, resulting in selective eating and consequently inadequate nutrient consumption.
Before the availability of pelleted diets, most birds were fed a seed mix that was high in fat and deficient in calcium, vitamin A, and other nutrients. The formulation of pelleted diets has significantly improved bird health. The recommended diet for larger parrots is 80% pellets with 10–15 % healthy vegetables and 5–10% fresh fruits. Seeds and nuts can be given occasionally as treats or for training. For most small birds (budgerigars, cockatiels, lovebirds), 40–50% pellets and 30–40% seed mix with 10–15% healthy vegetables and 5–10% fresh fruit is recommended.
Transitioning a Bird to a Pelleted Diet
Pet birds are often suspicious of anything new, so transition from seeds to pellets should be gradual. Pushing a bird to eat pellets too quickly can result in a thin, sick bird. Pellets should be introduced in a manner that allows the birds to become accustomed to the sight and taste of the pellets before the seed diet is completely removed. When beginning the transition, it is essential that owners monitor the bird's weight throughout the duration of the conversion. If the bird loses >10% of its body weight, the owner should call the veterinarian. If the owner cannot weigh the bird, the owner should monitor fecal output and call if it is reduced.
Ways to convert birds from seed diets to pellet diets:
Mix pellets and seeds together in a 20% pellet / 80% seed ratio for ~2 weeks. Then, increase the ratio of pellets to 30%, 50%, 75%, and 100%, with a 2-week interval between each stage.
Offer the new diet in the morning and throughout the day, when the bird is most hungry, and then offer the seed diet in the evening to be sure the bird is eating. Remove seed overnight.
Place a thin layer of pellets over the seed diet, to encourage the bird to pick through pellets, or sprinkle seed over the pellets to encourage the bird to eat through the upper layer of food to the pellets below.
Offer the new diet in the morning and evening while the family or owner is eating to encourage eating as a flock. Eating is a flock behavior in the wild. If one member in the flock starts eating, the others will often join in. Pretend to eat pellets in front of the bird and to enjoy them. Having your bird around other birds eating pellets will also help in conversion.
For birds who like to forage on the ground, place pellets on the ground or on a mirror on the bottom of the cage.
Moisten pellets, or cook pellets in corn bread or birdie bread, or place on rice, corn, or mixed veggies.
Important note: the above conversion programs should only be implemented with a bird that is not underweight and is not sick. If the bird is currently under veterinary care for an illness, do not start a conversion program.
For More Information
Also see pet health content regarding care and breeding of pet birds.





