




Vesicular adenitis or vesiculitis is inflammation and infection of one or both vesicular glands. There are no apparent or outward clinical signs, with the rare exception being the older bull that is chronically affected or has a peritonitis secondary to abscessation. Diagnosis typically occurs when the internal genitalia are examined via rectal palpation and microscopic evaluation of semen is performed as components of a breeding soundness examination. Although causative agents are sensitive to most broad-spectrum antimicrobials, only two macrolide compounds achieve necessary concentrations in the glands to be effective.
The vesicular glands (also sometimes referred to as "vesicles") are paired accessory sex glands located on the floor of the pelvis, lateral to the ampullae, and dorsal to the neck of the urinary bladder. They secrete a clear fluid that adds volume, nutrients, and buffers to semen but do not serve as a reservoir for spermatozoa (see urogenital tract photograph).

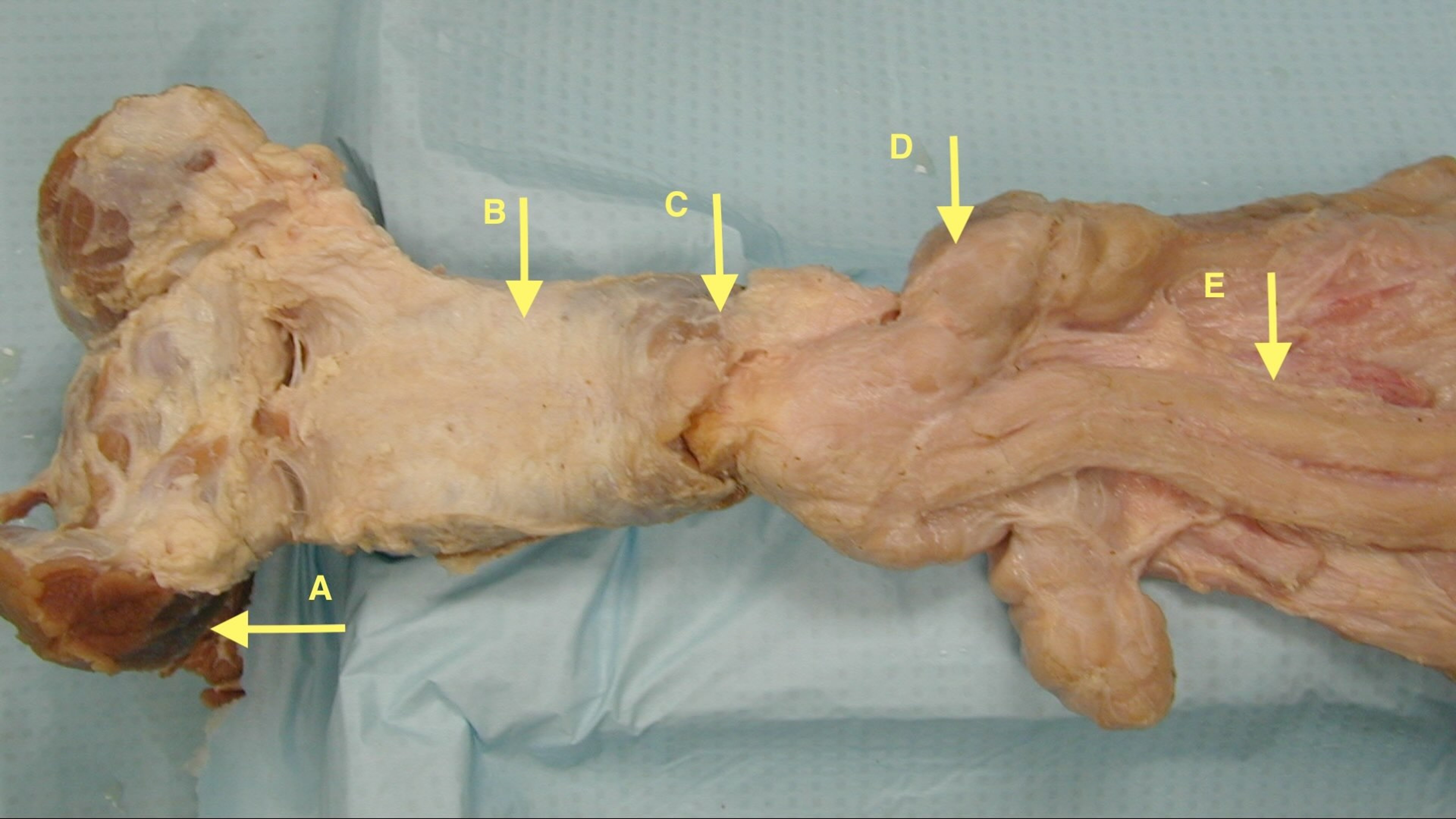
Courtesy of Dr. Ben Nabors.
Epidemiology of Vesicular Adenitis in Bulls
Vesicular adenitis has been reported in bulls wherever breeding cattle are raised, with the reported incidence being 1%–10%. A higher incidence is reported for young bulls developed on high-energy diets in group housing.
Etiology and Pathogenesis of Vesicular Adenitis in Bulls
In areas of the world without control measures in place for brucellosis, Brucella abortus is the primary cause of vesicular adenitis. Although a vast number and variety of organisms have been implicated, the following are the most commonly identified microbial pathogens:
Trueperella pyogenes
Pseudomonas aeruginosa
Streptococcus spp
Staphylococcus spp
Proteus spp
Escherichia coli
Mycoplasma bovis
Mycoplasma bovigenitalium
Historically, ascending, descending, or hematogenous routes of infection have been suggested. Of these, the hematogenous route is the most likely. Because there is an association between vesiculitis and high-energy diets, the following observations have been made:
A high-energy diet predisposes to rumen acidosis, which induces rumenitis, resulting in a bacteremia.
The same bacterial isolates that result in liver abscesses are found in infected vesicular glands.
A bacteremia after pneumonia, an unresolved umbilical infection, or other systemic infections are also possible etiologies.
The ascending route of infection, while possible, is unlikely unless the bull has accompanying penile trauma or urethritis. The descending route can be considered if the affected gland is ipsilateral to an infectious epididymitis or orchitis.
Congenital malformation of the excretory ducts of the vesicular glands where they open into the urethra at the colliculus seminalis has been reported. A malformation of the excretory duct orifice permits reflux of spermatozoa or urine from the pelvic urethra into the vesicular gland. If the tubular lining of the gland degenerates subsequent to irritation from abnormal material in the ducts, substantial local inflammation can result. This noninfectious etiology may account for the poor therapeutic response in some cases.
Clinical Findings of Vesicular Adenitis in Bulls
There are usually no outwardly observable clinical signs of vesicular adenitis. It has been suggested that a bull with a severe acute case or vesicle abscessation may stand with its back arched, have pain on defecation or rectal examination, and show hesitation when mounting. However, such clinical signs are very uncommon.
Diagnosis of Vesicular Adenitis in Bulls
Purulent material in semen
Rectal palpation of the vesicles
Rectal ultrasonography
Vesicular adenitis is most often diagnosed during a routine breeding soundness examination (BSE).
During rectal palpation for the evaluation of the internal genitalia, asymmetry in the size of the glands can be noted (see unilateral vesiculitis photograph).
One or both glands may be enlarged and indurated with loss of lobulation.


Courtesy of Dr. Donald R. Monke.
Bilateral vesiculitis is less common and may be difficult to diagnose because both vesicles may be equally large. It is possible for a gland to abscess, and in such cases, the affected vesicle is markedly larger than the other and may be fluctuant on palpation (see abscess photograph).


Courtesy of Dr. Donald R. Monke.
Rectal examination typically reveals an enlarged, sometimes irregular, and often fibrotic gland. Ultrasonographic diagnosis may include observation of enlarged glands, excess soft tissue opacities, or purulent material within the vesicles. Asymmetry of the vesicles can be detected by measuring the length and diameter of each gland during ultrasonographic examination.
During a correctly performed BSE, microscopic evaluation of sperm morphology is performed. Bulls with vesicular gland infection will have white cells in their ejaculate and thus present on the semen smear. Semen is typically stained with eosin-nigrosin, which does not highlight the WBCs (see eosin-nigrosin stain photomicrograph). They will appear as unstained round cells that have a diameter of > 2X that of a sperm head.


Courtesy of Dr. Jessica Cowley.
To confirm their identification, make another semen smear and stain with modified Giemsa stain (see modified Giemsa stain photomicrograph). It should be noted that the presence of 3–5 WBCs/high-powered field is indicative of infection, even without concurrent glandular swelling.

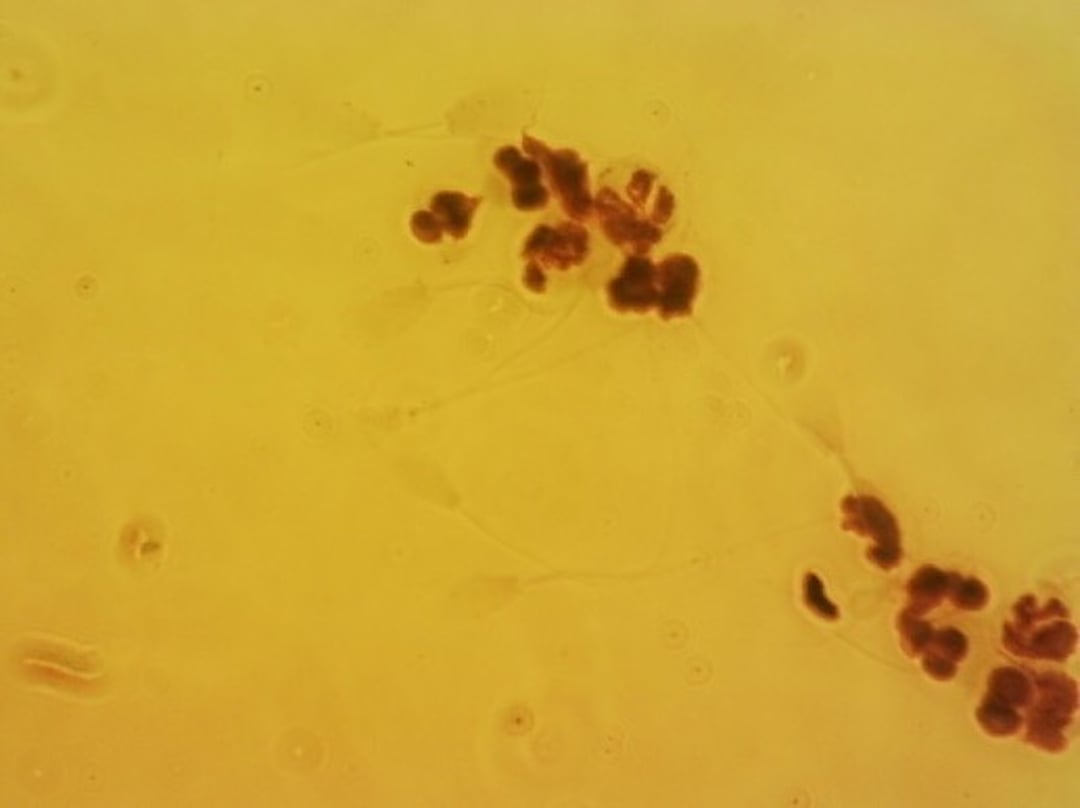
Courtesy of Dr. Jessica Cowley.
Transrectal ultrasonography is valuable both for confirmation of an enlarged vesicular gland and for the identification of abscessation.
Treatment and Prognosis of Vesicular Adenitis in Bulls
Systemic antimicrobial injection
Intraglandular injection for nonresponders
Although most of the likely pathogens in vesicular adenitis are sensitive to most broad-spectrum antimicrobials, they do not reach satisfactory levels even when administered at twice the label dosages. Only the macrolides, tulathromycin and tilmicosin, have been proven effective. Spontaneous remission may also occur in young bulls less than 18 months old.
Systemic treatment consists of a single injection of tulathromycin (2.5 mg/kg, SC, once) or tilmicosin (10 mg/kg, SC, once). In bulls that are not responsive to alternating rounds of the two macrolide antimicrobials, intraglandular injection of an antimicrobial is recommended if owners choose to attempt another treatment rather than culling. The drug of choice would be a broad-spectrum antimicrobial, such as ampicillin trihydrate.
To accomplish an intraglandular injection, the perineal area of the bull is cleaned with a surgical scrub, a hand is introduced into the rectum, and a 2.5- to 5-cm 14-gauge needle is placed into the skin lateral to the rectum. This needle assists in the introduction of a 20-cm-long 18-gauge needle that is directed toward and into the affected gland. This is facilitated by the hand holding the gland in place (see intraglandular injection photograph).
Any broad-spectrum antimicrobial can be used, and a volume sufficient to create swelling of the gland is recommended. Although leakage is not common, an antimicrobial that would not be irritating in the abdomen should be chosen. Administration by this method is considered extra-label drug use in the US. Tilmicosin should not be used, both because it would be irritating and because inadvertent puncture of the palpation hand is possible, risking severe injury or death to the human administering the drug. Also, this treatment is not effective once abscessation is present.


Courtesy of Dr. Josh Thompson.
Surgical excision of the affected gland is also a potential treatment. It is a difficult procedure and may affect semen quality due to decreased seminal fluid postoperatively. The prognosis after surgery is fair in yearling bulls; surgery has not been successful in chronically affected adult bulls.
See Pharmacotherapeutics in Seminal Vesiculitis in Bulls in Systemic Pharmacotherapeutics of the Urinary System for pharmacological considerations.
Key Points
Vesicular adenitis is often suspected in yearling bulls when white blood cells are observed during microscopic evaluation of the semen smear and/or rectal palpation of enlarged vesicles during a breeding soundness examination.
Treatment is aimed at eliminating the infection by systemic administration of prolonged-release broad-spectrum antimicrobials.
Contaminated semen is not suitable for artificial insemination and bulls with vesicular adenitis are considered unsatisfactory breeders until resolution is confirmed. Culling is recommended for bulls that do not recover.
For More Information
Hopper RM, ed. Bovine Reproduction. 2nd ed. John Wiley & Sons; 2021. doi:10.1002/9781119602484




