



Hypercalcemia is diagnosed when calcium is elevated outside of normal reference ranges. This usually indicates an underlying disease process causing the dysregulation of calcium homeostasis; clinical signs may or may not be evident.
The physiologic response to hypercalcemia is to:
decrease parathyroid hormone (PTH) secretion
increase calcitonin secretion
decrease calcitriol synthesis
Several diseases cause failure of these feedback mechanisms to properly lower the calcium concentration back into reference range.
Although there are many causes of hypercalcemia in animals, the most common causes in dogs include paraneoplastic hypercalcemia of malignancy, primary hyperparathyroidism, renal disease, and Addison disease. Please see the for a list of differential diagnoses.
Clinical Signs of Hypercalcemia in Dogs and Cats
Clinical signs of hypercalcemia can vary in their severity and progression. Marked elevations in calcium (> 14 mg/dL) and acute or rapid rises in calcium can result in more severe clinical signs. The disease process causing hypercalcemia may also contribute to additional clinical signs.
Clinical Signs Associated with Hypercalcemia
Body System | Descriptions |
|---|---|
Nervous | Weakness, lethargy, difficulty rising, trembling |
Gastrointestinal | Hyporexia, nausea, vomiting, constipation |
Urinary | Polydipsia, polyuria, urolithiasis, urinary tract infection |
Cardiovascular | Hypertension, arrhythmia |
Hypercalcemia is now frequently diagnosed in clinically normal patients based on routine pre-anesthetic or annual bloodwork. Up to one-third of patients with primary hyperparathyroidism (PHPT) had no clinical signs of hypercalcemia at the time of diagnosis.(1)
Hypercalcemia generally affects the nervous, gastrointestinal, and urinary systems. Please see the for a complete list of clinical signs.
Total calcium concentrations exceeding 15–18 mg/dL may be associated with systemic clinical signs that can be life-threatening. Goals of acute treatment of hypercalcemia include relieving symptoms, allowing diagnostic evaluation, and preventing death.
It is very important to treat the underlying condition. Intravenous fluid treatment using normal saline will promote calciuresis. Additional treatments that can be administered in an acute hypercalcemic crisis include furosemide, steroids, bisphosphonates, calcitonin, bicarbonate, and plicamycin. The selection of treatment should be based on the patient and on the severity and cause of the hypercalcemia. Additionally, dialysis can be used to lower calcium.
Note that any elevation in calcium concentration can be important, even when found incidentally, and warrants further evaluation.
Diagnosis of Hypercalcemia in Dogs and Cats
Common Diagnostic Tests in Veterinary Patients with Hypercalcemia
Diagnostic Test | Potential Abnormalities with Hypercalcemia |
|---|---|
Physical examination | Peripheral lymph node and anal sac assessment |
Chemistry | Calcium, phosphorus, renal values, electrolytes |
Urinalysis | USG, calcium oxalate crystals, bacteria |
Urine culture | Infection |
PTH, PTHrP, ionized calcium | May be normal, decreased or increased |
Abdominal radiograph | Bladder or kidney stones |
Thoracic radiographs | Metastasis, cranial mediastinum, thoracic lymph nodes |
Cervical ultrasonography | Enlarged parathyroid gland |
PTH, parathyroid hormone; PTHrP, parathyroid hormone-related protein; USG, urine specific gravity | |
A standard diagnostic database for hypercalcemia includes:
full physical examination with careful palpation of the peripheral lymph nodes
rectal examination with expression of the anal sacs to rule out apocrine gland anal sac adenocarcinoma
complete blood count
biochemical profile along with an ionized calcium test, which is the most accurate way of assessing a patient's calcium status
urinalysis and potentially a culture due to the high incidence of urinary tract disease
If hypercalcemia is noted on a clinically normal patient, a fasting blood sample can be resubmitted to help rule out a spurious result. Alternatively or if the hypercalcemia is repeatable, ionized calcium should be measured, because it reflects the biologically active form of calcium. Total calcium and adjusted total calcium are not reliable measurements of calcium status.
If ionized calcium is normal, even if total calcium is increased, a recheck of ionized calcium should be performed in 2–3 months. If ionized calcium is increased, then PTH and PTHrP determinations should be considered if there are no obvious causes of the hypercalcemia noted on physical examination.
Diagnoses for Hypercalcemia in Small Animals
Differential Diagnoses for Hypercalcemia | Descriptions |
|---|---|
Paraneoplastic hypercalcemia of malignancy | Apocrine anal sac adenocarcinoma, lymphoma, thymoma, carcinoma, others |
Primary hyperparathyroidism | Adenoma, hyperplasia, carcinoma |
Renal failure | Acute or chronic |
Medications | Thiazide diuretics, vitamin D toxicosis, calcium supplementation, vitamin A toxicosis |
Granulomatous disease | Fungal disease, panniculitis, injection reaction |
Nonparathyroid endocrine | Hypoadrenocorticism, thyrotoxicosis |
Skeletal disease | Osteomyelitis, osteoporosis, hypertrophic osteodystrophy |
Toxic | House plants, rodenticides, raisin/grape |
Transient | Associated with hemoconcentration, hyperproteinemia |
Idiopathic | Cats only |
Spurious | Lab error, tube or sample error |
Nonpathologic | Postprandial, young age, lipemia |
Parathyroid hormone and parathyroid hormone–related protein concentrations should be evaluated concurrently with ionized calcium. This relationship is dynamic, and therefore it is important to see the PTH concentration in the face of the calcium concentration. Normally, hypercalcemia should cause low or nondetectable PTH. Therefore, an increased ionized calcium concentration with a concurrent normal or increased PTH concentration is consistent with a diagnosis of PHPT.
Anticipated Laboratory Results for Different Causes of Hypercalcemia
Ionized Calcium | Total Calcium | PTH | PTHrP | Phosphorus | Calcidiol | Calcitriol | |
|---|---|---|---|---|---|---|---|
Granulomatous | ↑ | ↑ | ↓N | ↑N | ↑N | N | ↑N |
Osteolytic | ↑ | ↑ | ↓ | ↑N | ↑N | N | N |
PHPT | ↑ | ↑ | ↑N | N | ↓N | N | ↑N |
Vitamin D toxicosis | ↑ | ↑ | ↓ | N | ↑ | N | ↑ |
Addison | ↑ | ↑ | ↓N | N | ↑N | N | ↓N |
Acute renal disease | ↑ | ↑ | ↓N | N | ↑N | N | ↓N |
Chronic renal disease | ↓N | ↑↓N | ↑ | N | ↑N | ↓N | ↓N |
Nutritional | ↓N | ↓N | ↑ | N | ↑N | ↓N | ↓N |
Tertiary HPT | ↑ | ↑ | ↑ | N | ↑ | ↓N | ↓N |
Neoplasia | ↑ | ↑ | ↓N | ↑N | ↓N | N | ↑↓N |
Idiopathic | ↑ | ↑ | ↓N | N | ↑N | ↓N | ↑↓N |
Determining the etiology of hypercalcemia can be challenging: one study found that 75% of dogs with confirmed PHPT had PTH concentrations within reference ranges.(1) However, PTHrP concentrations can also be increased, as in patients with humoral hypercalcemia of malignancy.
Vitamin D status can be assessed by measuring calcidiol and calcitriol concentrations. Because vitamin D metabolites play a role in calcium homeostasis, assessing vitamin D status should be considered when creating a diagnostic plan.
Vitamin D metabolites resulting from ingesting cholecalciferol present in rodenticides can be measured with the calcidiol assay. Toxicity from ingestion of cholecalciferol or ergocalciferol would be detected by an increase of calcidiol that may persist for weeks after exposure. Assay of calcidiol also may be used to confirm toxicity from ingestion of rodenticides that contain vitamin D3 as the active ingredient.
Imaging of the abdomen and thorax is warranted in patients with hypercalcemia. Abdominal radiographs or ultrasound examination should be performed to rule out urolithiasis. Thoracic radiographs are used to evaluate the lungs for evidence of masses or metastasis, thoracic lymph nodes, the cranial mediastinum, and bones in the field of view for osteolytic lesions.
Primary Hyperparathyroidism
Primary Hyperparathyroidism in Dogs
Primary hyperparathyroidism occurs when single or multiple parathyroid glands become hyperfunctional and autonomously secrete PTH, losing normal responses to negative feedback. Hyperfunctional activity can be caused by solitary adenoma (most common), multiple adenomas, hyperplasia or carcinoma.
There are hereditary causes of PHPT in humans and dogs. Keeshonds have an autosomal dominant mode of inheritance, and genetic testing can be performed at Cornell University's Animal Health Diagnostic Center. Most dogs are older than 7 years when they develop this disease, and there is no sex predilection.
Besides Keeshonds, other breeds that are overrepresented include Labrador Retrievers, German Shepherd Dogs, Golden Retrievers, Poodles, Shih Tzus, Springer Spaniels, Australian Shepherds, Cocker Spaniels, Rhodesian Ridgebacks, Lhasa Apsos, Doberman Pinschers, and mixed-breed dogs.
Dogs with PHPT tend to have mild clinical signs in general, but can sometimes be quite sick at presentation. Urinary signs seem to be the most common, with 31% of patients having urolithiasis and 29% having urinary tract infections. Dogs with PHPT form calcium oxylate stones from hypercalcemia and calciuresis. The stones can be a nidus for infection and urinary tract infections. Other commonly reported clinical signs include polyuria, polydipsia, weakness, lethargy, hyporexia, weight loss, vomiting, and tremors.


Lateral radiograph of a dog with primary hyperparathyroidism as well as calcium oxalate bladder stones.
Lateral radiograph of a dog with primary hyperparathyroidism as well as calcium oxalate bladder stones.
Courtesy of Dr. Kathleen Ham.

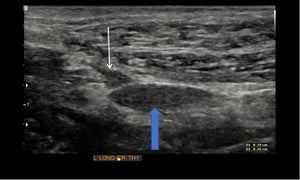
Longitudinal ultrasonographic image of the thyroid and a parathyroid nodule. Cranial is to the left. The large block blue arrow is pointing towards the thyroid lobe. The small white arrow is pointing to the round parathyroid nodule measuring 0.19 cm × 0.26 cm.
Longitudinal ultrasonographic image of the thyroid and a parathyroid nodule. Cranial is to the left. The large block bl
Courtesy of Dr. Kathleen Ham.


Transverse ultrasonographic image of the parathyroid nodule; lateral is to the right. The large block blue arrow is pointing towards the trachea. The small white arrow is pointing to the hypoechoic round parathyroid nodule measuring 0.19 cm × 0.22 cm
Transverse ultrasonographic image of the parathyroid nodule; lateral is to the right. The large block blue arrow is poi
Courtesy of Dr. Kathleen Ham.

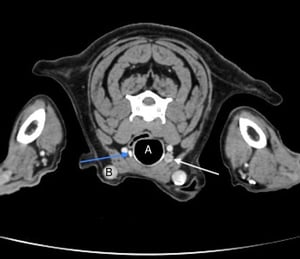
Transverse or axial CT image of a dog with a large parathyroid nodule. The letter A is the trachea and B is the external jugular vein. The white arrow is pointing towards the parathyroid nodule and the blue arrow is pointing to the normal contralateral thyroid lobe.
Transverse or axial CT image of a dog with a large parathyroid nodule. The letter A is the trachea and B is the externa
Courtesy of Dr. Kathleen Ham.

Dorsal CT image of a dog with a large parathyroid nodule. The letter A is the trachea. The white arrow is pointing to the parathyroid nodule and the blue arrows are pointing to the thyroid lobes.
Dorsal CT image of a dog with a large parathyroid nodule. The letter A is the trachea. The white arrow is pointing to t
Courtesy of Dr. Kathleen Ham.

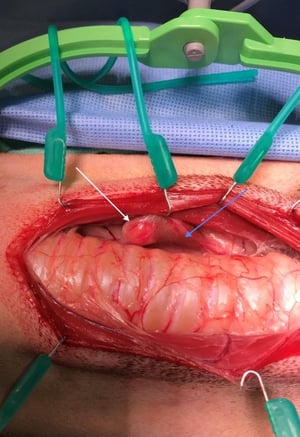
Intraoperative photograph of a parathyroidectomy in a dog. Cranial is to the right. The incision is being retracted with a ring retractor. The trachea is exposed. The white arrow points to the parathyroid nodule and the blue arrow points to the thyroid lobe.
Intraoperative photograph of a parathyroidectomy in a dog. Cranial is to the right. The incision is being retracted wit
Courtesy of Dr. Kathleen Ham.


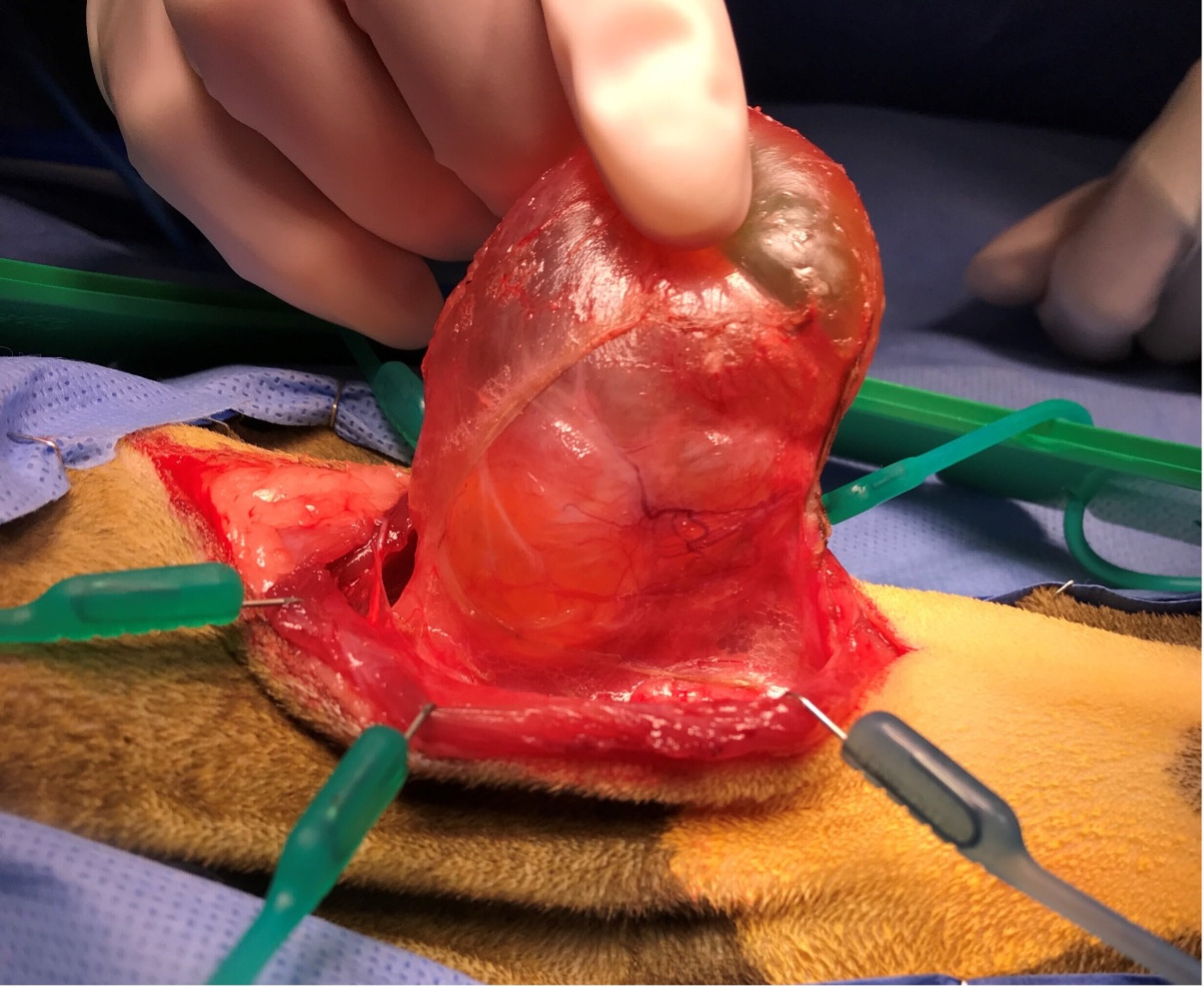
Image of excised thyroid and parathyroid in a dog. Cranial is to the left. The white arrow points to the parathyroid nodule. The blue arrow points to the thyroid lobe. The thyroid was removed in addition to the parathyroid due to a thyroid nodule found at surgery.
Image of excised thyroid and parathyroid in a dog. Cranial is to the left. The white arrow points to the parathyroid no
Courtesy of Dr. Kathleen Ham.


Excised parathyroid nodule from a dog. The nodule is large and round.
Excised parathyroid nodule from a dog. The nodule is large and round.
Courtesy of Dr. Kathleen Ham.


A dog with full thickness necrosis of the skin overlying a lateral saphenous intravenous catheter site, as a result of extravasation of calcium-containing fluids.
A dog with full thickness necrosis of the skin overlying a lateral saphenous intravenous catheter site, as a result of
Courtesy of Dr. Kathleen Ham.
Lateral radiograph of a dog with primary hyperparathyroidism as well as calcium oxalate bladder stones.
Lateral radiograph of a dog with primary hyperparathyroidism as well as calcium oxalate bladder stones.
Courtesy of Dr. Kathleen Ham.
Longitudinal ultrasonographic image of the thyroid and a parathyroid nodule. Cranial is to the left. The large block blue arrow is pointing towards the thyroid lobe. The small white arrow is pointing to the round parathyroid nodule measuring 0.19 cm × 0.26 cm.
Longitudinal ultrasonographic image of the thyroid and a parathyroid nodule. Cranial is to the left. The large block bl
Courtesy of Dr. Kathleen Ham.
Transverse ultrasonographic image of the parathyroid nodule; lateral is to the right. The large block blue arrow is pointing towards the trachea. The small white arrow is pointing to the hypoechoic round parathyroid nodule measuring 0.19 cm × 0.22 cm
Transverse ultrasonographic image of the parathyroid nodule; lateral is to the right. The large block blue arrow is poi
Courtesy of Dr. Kathleen Ham.
Transverse or axial CT image of a dog with a large parathyroid nodule. The letter A is the trachea and B is the external jugular vein. The white arrow is pointing towards the parathyroid nodule and the blue arrow is pointing to the normal contralateral thyroid lobe.
Transverse or axial CT image of a dog with a large parathyroid nodule. The letter A is the trachea and B is the externa
Courtesy of Dr. Kathleen Ham.
Dorsal CT image of a dog with a large parathyroid nodule. The letter A is the trachea. The white arrow is pointing to the parathyroid nodule and the blue arrows are pointing to the thyroid lobes.
Dorsal CT image of a dog with a large parathyroid nodule. The letter A is the trachea. The white arrow is pointing to t
Courtesy of Dr. Kathleen Ham.
Intraoperative photograph of a parathyroidectomy in a dog. Cranial is to the right. The incision is being retracted with a ring retractor. The trachea is exposed. The white arrow points to the parathyroid nodule and the blue arrow points to the thyroid lobe.
Intraoperative photograph of a parathyroidectomy in a dog. Cranial is to the right. The incision is being retracted wit
Courtesy of Dr. Kathleen Ham.
Image of excised thyroid and parathyroid in a dog. Cranial is to the left. The white arrow points to the parathyroid nodule. The blue arrow points to the thyroid lobe. The thyroid was removed in addition to the parathyroid due to a thyroid nodule found at surgery.
Image of excised thyroid and parathyroid in a dog. Cranial is to the left. The white arrow points to the parathyroid no
Courtesy of Dr. Kathleen Ham.
Excised parathyroid nodule from a dog. The nodule is large and round.
Excised parathyroid nodule from a dog. The nodule is large and round.
Courtesy of Dr. Kathleen Ham.
A dog with full thickness necrosis of the skin overlying a lateral saphenous intravenous catheter site, as a result of extravasation of calcium-containing fluids.
A dog with full thickness necrosis of the skin overlying a lateral saphenous intravenous catheter site, as a result of
Courtesy of Dr. Kathleen Ham.
Up to one-third of dogs may be clinically normal, and the diagnosis of hypercalcemia is found incidentally. Physical examination findings tend to be unremarkable, and the actual palpation of a nodule is very unlikely.
Once a diagnosis of PHPT is suspected, localization tests can be used to detect the abnormal gland(s) as well as help prepare for surgery. Cervical ultrasonography is the localization technique most commonly used but requires an experienced ultrasonographer because abnormal glands can be as small as 4 mm.
Other imaging techniques (CT, MRI, and nuclear scintigraphy) can be considered for evaluation of the parathyroid glands, but have lower sensitivity for this purpose than does ultrasonography.
Treatment and Prognosis
Treatment for PHPT is highly effective and should be strongly recommended even in older dogs. The most common and effective treatment method is surgical excision of the hyperfunctional parathyroid gland(s). The surgical cure rate is 95%, and success rates are dependent on surgeon experience.
An alternative to surgery is ultrasound-guided glandular ablation by radiofrequency or ethanol injection. The cure rates are ~90%, but the patient still requires general anesthesia and may need multiple treatments. A common misconception is that patients may be too old for surgery; however, if the surgery is being performed by an experienced clinician, the anesthetic time is low.
Postoperative hypocalcemia is common, necessitating ongoing treatment and, in some cases, prolonged hospitalization. Several retrospective studies have tried to identify variables associated with the risk of developing hypocalcemia after surgery; patients with a total calcium concentration > 14mg/dL are reported to be at greater risk.(2,3)
Newer studies have found additional variables associated with the development of hypocalcemia after parathyroidectomy: older age, history of weakness, high serum BUN concentrations, preoperative PTH serum concentrations above reference range, and low calcium phosphorus product.(4, 5) Additionally, patients may have a higher risk if the initial ionized calcium (iCa) concentrations are greater than 1.75 mmol/L.(6, 7)
Some surgeons opt for prophylactic enteral calcitriol supplementation or calcium carbonate supplementation, but a protective effect has not been demonstrated in the literature thus far.(8)
Treatment of hypocalcemia after surgery is best done enterally with calcitriol. During a hypocalcemic crisis, parenteral calcium supplementation must also be used but may be associated with several complications—most notably, arrhythmias and severe tissue injury if extravasated.
The other major complication associated with treatment is failure to resolve the hypercalcemia. Causes of persistent hypercalcemia include surgeons mistaking thyroid pathology for the parathyroid nodule, patients having multiglandular disease and missing additional parathyroid pathology at the initial surgery, or the tissue being ectopic.
Primary Hyperparathyroidism in Cats
Primary hyperparathyroidism is less common in cats than in dogs: the largest current retrospective study contains only 32 cats over 12 years from 10 different referral hospitals.(8) As in dogs, the most common histopathologic finding is adenoma; however, carcinoma is also possible. Additionally, parathyroid masses in cats may have larger cystic components.

Intraoperative photograph of a parathyroid cyst in a cat.
Courtesy of Dr. Kathleen Ham.
The prognosis in cats is very good with surgical removal of the hyperfunctional gland, and therefore surgery should be recommended.
Key Points
Most animals with PHPT are older.
Bladder stones and UTIs are fairly common with PHPT.
Abnormal parathyroid tissue may be very small, ectopic, or multiglandular; ultrasonography is most often used for localization.
Treatment of PHPT is very successful, although transient hypocalcemia after surgery is common.
PHPT is rare in cats. Cats may have cystic components of the parathyroid mass.
Other Common Causes of Hypercalcemia
Paraneoplastic (Humoral) Hypercalcemia of Malignancy in Dogs and Cats
Humoral hypercalcemia of malignancy is the most common cause of hypercalcemia in dogs and is common in cats. Many patients with hypercalcemia due to malignancy are sick from the hypercalcemia and sometimes from the cancer. Parathyroid hormone-related protein acts on PTH receptors in the kidney to increase calcium resorption and phosphorus excretion. It also increases osteoclastic bone resorption.
Patients suffering from dehydration and renal insufficiency may develop hypercalcemia faster and become sicker due to the decreased renal calcium excretion.
The two most common cancers that cause humoral hypercalcemia of malignancy in dogs are lymphoma and apocrine gland anal sac adenocarcinoma, although almost any cancer can cause hypercalcemia of malignancy. In cats, the two most common cancers are lymphoma and squamous cell carcinoma. Humoral hypercalcemia of malignancy can be caused by PTHrP, but other factors include transforming growth factor, vitamin D metabolites, cytokines and others. Therefore, even if PTHrP concentrations are not detectable, a malignant process is not ruled out.
Addison Disease in Dogs and Cats
Hypercalcemia may occur in up to ~30% of patients with hypoadrenocorticism, or Addison disease; however, it is usually transient and resolves when the patient is treated with volume re-expansion, steroids, and, if needed, mineralocorticoids. The hypercalcemia can be mild, and the ionized calcium is usually normal.
Secondary and Tertiary Hyperparathyroidism in Dogs and Cats
Secondary hyperparathyroidism (SHPT) is characterized by increased PTH concentrations and low or normal calcium. Conditions that lead to SHPT include renal failure, vitamin D deficiency, decreased calcium intake, and malabsorption.
Animals with chronic renal failure can develop renal secondary hyperparathyroidism due to complex interactions of ionized calcium, phosphorus, vitamin D metabolites, PTH, and fibroblast growth factor. These patients have changes in phosphorus retention, decreased calcitriol synthesis, and hypocalcemia. Secondary hyperparathyroidism occurs in response to prolonged states of hypocalcemia, and the important difference is that the parathyroid glands are normal. Calcitriol can be an effective treatment to decrease PTH concentrations and improve quality of life in many of these patients.
Nutritional secondary hyperparathyroidism occurs with vitamin D deficiency and in patients fed diets with no or low calcium. When the diet is void of vitamin D, there is diminished intestinal calcium absorption, leading to decreased extracellular calcium. Decreased extracellular calcium will drive increased PTH synthesis and secretion. Because there is not a dietary source of calcium, the PTH will pull calcium from the skeletal reserves, resulting in altered bone metabolism.
Tertiary hyperparathyroidism (THPT) is a condition reflecting the development of abnormal parathyroid function after a period of secondary hyperparathyroidism, resulting in increased concentrations of PTH and ionized calcium. Patients with THPT typically have hypercalcemia, hyperphosphatemia, and increased PTH concentrations. Surgery to remove some or all of the parathyroid glands may be recommended. Medications such as cinacalcet, a calcimimetic, have also been used in humans.
Idiopathic Hypercalcemia in Cats
The most common form of hypercalcemia in cats is idiopathic, which leads to a mild to moderate hypercalcemia and rarely a severe hypercalcemia. Most cats with hypercalcemia are middle-aged, but it can occur at any age with no sex predilection, and long-haired cats seem to be overrepresented. Proposed causes include genetic factors and the use of acidifying diets, which result in a chronic metabolic acidosis and resultant bone resorption.
Many cats with idiopathic hypercalcemia (IHC) have no clinical signs; however, hypercalcemia generally causes anorexia and weight loss in cats and the other clinical signs listed in the . Because a diagnosis of IHC is a diagnosis of exclusion, the minimum database usually includes a complete blood count, serum biochemistry, iCa, PTH malignancy panel, urinalysis, and thorax and abdominal imaging to evaluate for neoplasia and urolithiasis. Additionally, vitamin D metabolites and cervical imaging should also be considered.
Treatment recommendations are based on the presence or absence of clinical signs, presence of urinary stones and the severity of the hypercalcemia. Management considerations for IHC include diet changes, such as nonacidifying diets, canned diets, and fiber supplementation, as well as medications such as steroids and bisphosphonates.
Key Points
Paraneoplastic syndrome, hypoadrenocorticism, nutritional deficiencies and renal disease are other common causes of hypercalcemia in dogs and cats.
The cancers most commonly associated with hypercalcemia are lymphoma, anal gland adenocarcinoma (dogs) and squamous cell carcinoma (cats).
Hypercalcemia in cats is most often idiopathic.
Nutritional history is important when evaluating patients with abnormal calcium.
Hypoparathyroidism
Hypoparathyroidism is a condition manifested by low or absent PTH concentrations in the face of low calcium concentrations. Causes of hypoparathyroidism include surgical excision, trauma, spontaneous, idiopathic, immune mediated, abnormal magnesium concentration, drug reaction, malignancy, radiation, and hungry bone syndrome. Clinical signs are manifestations of low serum calcium concentrations and include nervousness, seizures, muscle fasciculations, muscle twitching, muscle cramping, facial rubbing, weakness, inappetence, and ataxia.
If hypoparathyroidism is suspected, a thorough history should be obtained, including recent surgery, medications, and diet. Calcium, ionized calcium, phosphorus, vitamin D metabolites and PTH concentrations should be evaluated.
Treatment is based on the patient's overall status and clinical signs. Those patients with severe clinical signs will require parenteral calcium supplementation either as bolus or constant-rate infusion until stable. Patients with mild clinical signs should receive enteral calcitriol and calcium supplementation. If the patient has vitamin D or magnesium deficiency those should also be corrected.
If the hypoparathyroidism is due to recent surgery, then PTH concentrations should return to normal within 6 months of the procedure. Longterm management is sometimes required however, involving lifelong supplementation, monitoring and good owner communication.
Parenteral Calcium Administration
Hypocalcemic tetany or convulsions are indications for the immediate IV administration of 10% calcium gluconate (1–1.5 mL/kg, equivalent to 5-15 mg/kg of elemental calcium), which should be slowly infused over 10-30 minutes. Close monitoring is mandatory; if bradycardia or shortening of the QT interval occurs, the IV infusion should be slowed or temporarily discontinued.
References
Feldman EC, Hoar B, Pollard R, Nelson RW. Pretreatment clinical and laboratory findings in dogs with primary hyperparathyroidism: 210 cases (1987-2004). J Am Vet Med Assoc. 2005;227(5):756-761. doi:10.2460/javma.2005.227.756
Feldman EC, Miner A. Canine and Feline Endocrinology. 4th ed. Elsevier; 2015.
Ettinger SJ, Feldman EC. Textbook of Veterinary Internal Medicine: Diseases of the Dog and the Cat. 7th ed. Elsevier Saunders; 2010.
Milovancev M, Schmiedt CW. Preoperative factors associated with postoperative hypocalcemia in dogs with primary hyperparathyroidism that underwent parathyroidectomy: 62 cases (2004-2009). J Am Vet Med Assoc. 2013;242(4):507-15. doi:10.2460/javma.242.4.507
Burkhardt SJ, Sumner JP, Mann S. Ambidirectional cohort study on the agreement of ultrasonography and surgery in the identification of parathyroid pathology, and predictors of postoperative hypocalcemia in 47 dogs undergoing parathyroidectomy due to primary hyperparathyroidism. Vet Surg. 2021;50(7):1379–1388. doi:10.1111/vsu.13707
Dear JD, Kass PH, Della Maggiore AM, Feldman EC. Association of hypercalcemia before treatment with hypocalcemia after treatment in dogs with primary hyperparathyroidism. J Vet Intern Med. 2017;31(2):349-354. doi:10.1111/jvim.14644
Armstrong AJ, Hauptman JG, Stanley BJ, et al. Effect of prophylactic calcitriol administration on serum ionized calcium concentrations after parathyroidectomy: 78 cases (2005-2015). J Vet Intern Med. 2018;32(1):99-106. doi:10.1111/jvim.15028
Singh A, Giuffrida MA, Thomson CB, et al. Perioperative characteristics, histological diagnosis, and outcome in cats undergoing surgical treatment of primary hyperparathyroidism. Vet Surg. 2019;48(3):367-374. doi:10.1111/vsu.13165





