

Among the many disorders that can affect the foot of a horse are laminitis, navicular disease, puncture wounds, infections, keratoma, pedal osteitis, pyramidal disease, quittor, sandcrack, scratches, seedy toe, sheered heels, sidebone, thrush, bone cysts, bruises, corns, cankers, and fractures.
Anatomy of the horse’s foot

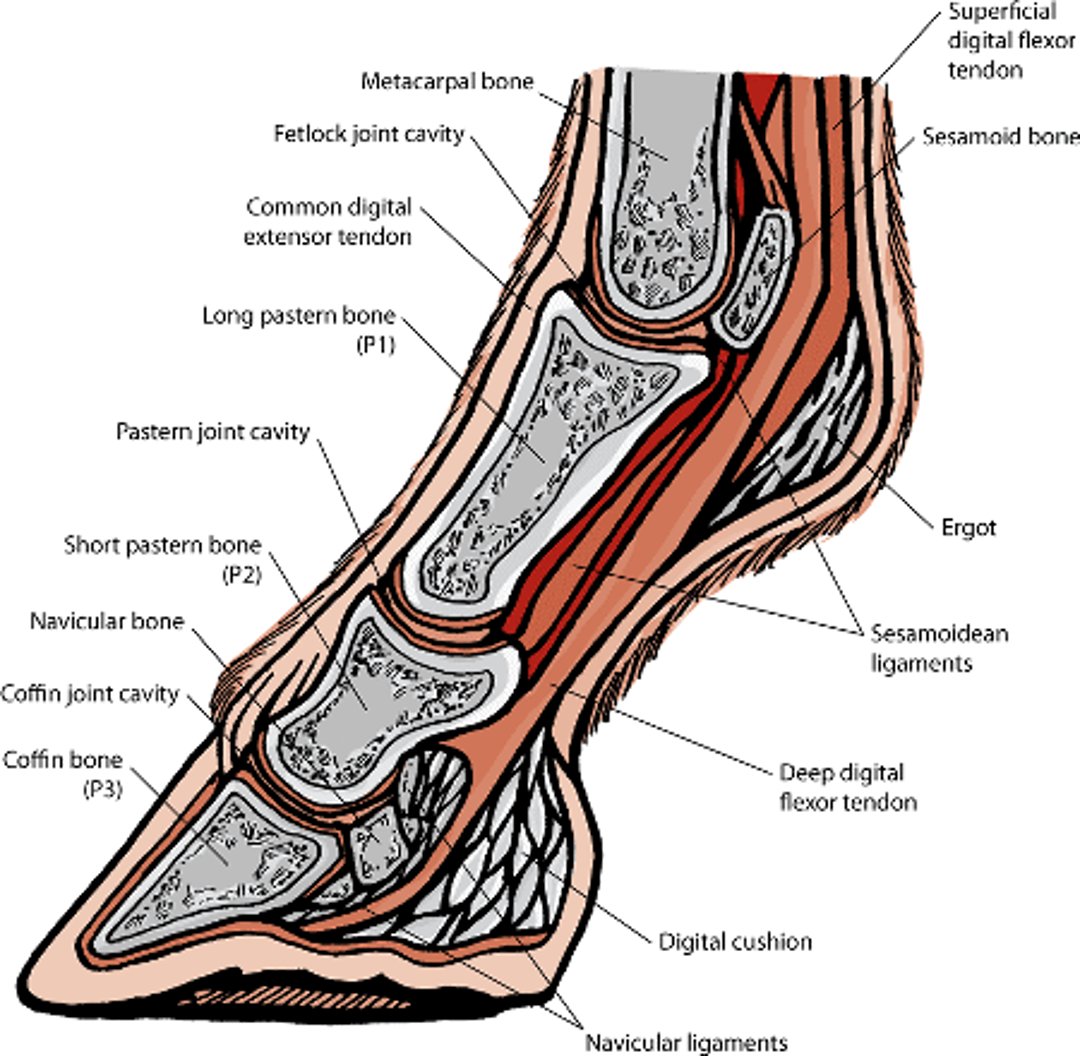
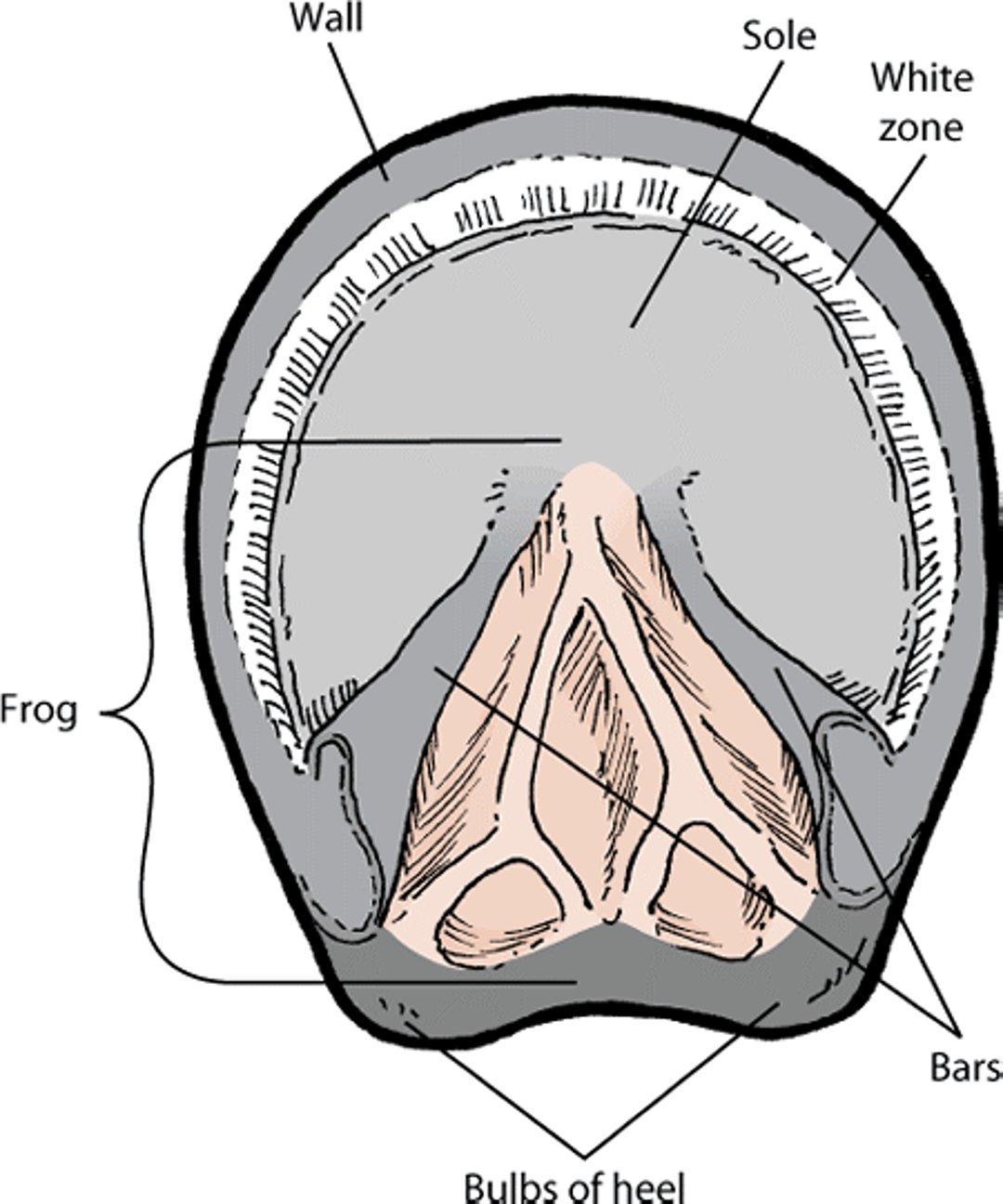
Hoof anatomy

Sole Bruises and Abscesses
Bruising on the sole of the foot usually is caused by direct injury from stones, irregular ground, or other trauma. Poor shoeing, especially in horses with flat feet or dropped soles, can increase the risk of bruising, usually around the outside edge of the sole or at the toe. Bruising may or may not be associated with lameness, depending on the severity. The sole may appear normal or may appear reddened or feel swollen or moist. If untreated, the affected area can become infected (a subsolar abscess).
A corn is a type of bruise that appears in the sole at the buttress (that is, the angle between the wall and the bar). It is most common in the forefeet on the inner buttress. Corns may arise from pressure applied to the sole by the heel of a shoe improperly placed or left on too long. Shoes that have been fitted too closely at the quarters or that are too small can also cause corns.
Foot abscesses, also called “sole abscesses” or “subsolar abscesses” are the most common cause of lameness in horses. Because horse’s hooves are exposed to mud, manure, and have tiny cracks from constant use, these areas of bacterial infection do occur. Lameness is often severe until the abscess ruptures or is opened to drain. Because the hooves are hard tissue, it can sometimes take several days or, in the worst cases, weeks for the infection to be cleared. Most abscesses are accessible from the sole, but some break out at the heel bulbs or the coronet. Careful palpation of the heels and coronet and the use of hoof testers to find a soft or painful spot in the sole can help to locate an abscess. Soaking the foot and pain medication are standard treatments. In cases of suspected foot abscess that are not resolving, xrays or more advanced imaging techniques may be required.
Canker
Canker is an overgrowth and infection of the horn-producing tissues (epithelium) of the foot. It involves the tough flexible pad in the middle of the sole (the frog) and the sole. Pus is usually obvious. The cause is unknown. Although frequently described as a disease seen in horses kept in moist or unsanitary environments, it is also encountered in well-cared-for horses.
Canker is found in both the front and hind feet. It usually starts at the back of the frog and appears as fronds or cauliflower-like growth. The affected tissues are usually covered by a thick, foul-smelling discharge. The disease may extend to the sole and even to the wall of the hoof and show no tendency to heal.
Treatment must be intensive. All loose horn and affected tissue should be removed, and an antiseptic or antibiotic dressing applied daily. A clean, dry wound environment must be maintained to allow healing, which may take weeks or months. Watch closely during the healing period to see whether any abnormal regrowth appears. If it does, it must be promptly treated.
Contracted Heels
Contracted heels are seen primarily in the forefeet of light horses. The condition may be caused by improper shoeing that draws in the quarters. This prevents hoof expansion and adequate frog pressure. Dry hooves, excess scraping of the wall, and trimming of the bars make a horse more prone to contracted heels. However, this condition may also occur after the use of a hoof-immobilizing shoe, such as that used for fracture of the third phalanx (coffin bone).
When the heel is contracted, the frog is narrow and shrunken, and the bars may be curved or almost parallel to each other. The quarters and heels are noticeably contracted and drawn in. The hoof horn is dry and hard, and heat may be noticed around the heels and quarters. If the horse is worked at speed, it may become lame, and its stride length will be shortened.
Treatment is by corrective trimming and shoeing, performed by your farrier in collaboration with your veterinarian. In advanced cases, recovery can take 6 to 12 months.
Fracture of the Coffin Bone
Coffin bone fractures generally occur at high speed (for example, during a race) or less commonly from kicking a firm object (such as the stall wall). The jarring injury produces a sudden onset of lameness. The lameness is severe if the fracture extends up into the adjacent joint. Fractures through the wing (flat side) of the coffin bone that do not involve the joint may produce less severe lameness. Coffin bone fractures occur more frequently in the forelimb but are also common in the hindlimb.
A horse that fractures its coffin bone immediately becomes lame. Compressing the foot with hoof testers causes pain. Lightly tapping the hoof with a hammer also may cause pain, and turning the horse or making it pivot on the affected leg worsens the lameness. Lameness may improve considerably after 48 hours of stall rest, unless the fracture extends into the joint.
Diagnosis is confirmed by regional analgesia and x-rays. X-ray confirmation may be difficult immediately after the injury because the fracture may be only a hairline at this stage. Repeating the x-ray several days or weeks later may be necessary for confirmation and to determine the extent of the fracture. If x-rays cannot confirm the presence of a fracture, scintigraphy or magnetic resonance imaging (MRI) may be necessary.
Conservative treatment of 6 to 9 months’ rest is usually all that is required for fractures that do not involve the joint. The horse should return to soundness, although the fracture will remain visible on x-rays. It is usual to fit a straight bar shoe with a clip well back on each quarter to limit expansion and contraction of the heels. In young horses (less than 3 years old), fractures into the joint usually heal satisfactorily, provided a 12-month rest period is given. Horses older than 3 years have a much less favorable outlook for recovery, and surgical insertion of a bone screw is recommended.
Keratoma
A keratoma is a hard, thickened area of the horn, located between the coffin bone and the hoof wall, usually at the toe. The cause is unknown. The condition usually forms at the level of the coronary band but may be difficult to detect until the growth is well advanced. Usually, there is bulging of either the coronary band or the hoof wall over the keratoma, depending on its position within the foot. Examining the surface of the underside of the horse’s forefoot shows that the growth has pushed the white line in toward the center of the sole. The pressure from the mass can shrink the coffin bone. Surgical removal of the mass is recommended.
Laminitis (Founder)
A horse’s foot has 2 types of laminae (tissue layers). The sensitive laminae are attached to the coffin bone. The insensitive laminae are the layers of tissue just inside the hard exterior of the hoof. The word laminitis means “inflammation of the laminae,” and it can refer to either a short-term (acute) inflammation or the disease caused by longterm or repeated (chronic) attacks of inflammation. Laminitis can develop in the forefeet, in all 4 feet, or in the hindfeet only. Supporting limb laminitis can be seen in a single foot, usually as a complication of a severe lameness or bone injury in the limb on the opposite side of the body.
Acute laminitis occurs when cells on the insensitive laminae fail to attach to the sensitive laminae. Because the laminae suspend the coffin bone within the hoof, failure of laminar attachments results in catastrophic displacement of the coffin bone. The heavy weight of the horse and the pull of the flexor tendons can contribute to the displacement. The coffin bone can rotate, sink, or tilt within the hoof. If rotation progresses, a hole may form through the sole of the foot.
Three disease states are thought to be associated with laminitis: 1) diseases that cause bacteria or bacterial toxins to spread through the blood (called sepsis and endotoxemia, respectively), 2) hormonal disorders (such as equine metabolic syndrome), and 3) pain or inability to use the limb on the other side of the body. The most common causes of laminitis are ingestion of too much grain, grazing of lush pastures (especially in ponies or overweight horses), and excessive exercise or repetitive trauma. Other causes include generalized infections, ingestion of black walnut heartwood shavings, retained placenta after delivery of a foal, colitis, colic, and treatment with corticosteroids and certain other medications. The risk is higher in ponies and in horses that are overweight and unfit. The number of cases of acute laminitis tends to increase whenever there is a flush of new grass.
Signs and Diagnosis
Laminitis is considered acute, subacute, or chronic. Acute laminitis is the first few days of founder before any displacement of the coffin bone occurs. Subacute laminitis is founder that has lasted longer than 3 days but still does not involve displacement of the coffin bone. Chronic laminitis describes horses with coffin bone displacement, regardless of how long ago the condition started.
In acute laminitis, the horse is depressed, has no appetite, and stands reluctantly. The horse resists exercise and attempts to shift weight off of the affected feet. If forced to walk, it has a slow, crouching, short-striding gait. Each foot, once lifted, is set down as quickly as possible.
Usually, heat is apparent in the whole hoof, especially near the coronary band. Pain can cause muscle trembling, and pressure reveals tenderness in the feet. Lameness is usually moderate to severe at this stage. X-ray evidence of rotation can be present as early as the third day. Horses with laminitis typically have elevated vital signs, such as increased body temperature, heart rate, and respiration. In exceptionally severe cases, for which the outlook for recovery is unfavorable, a blood-stained discharge may seep from the coronary bands.
In subacute cases, the horse may exhibit any or all of the above signs but to a lesser degree. Often, there is only a mild change in stance, with reluctance to walk and some increased sensitivity in the soles of the affected feet. Episodes of acute or subacute laminitis tend to come back at varying intervals and may develop into a chronic condition.
Horses with chronic laminitis are usually extremely lame and may spend a lot of time lying down. Longterm cases of chronic laminitis are characterized by changes in the shape of the hoof and usually follow one or more acute attacks. Bands of irregular horn growth (laminitic rings) may appear in the hoof, and the hoof itself may narrow and become elongated, with the wall almost vertical at the top (near the coronary band) and horizontal at the bottom (near the sole). As the condition progresses, the sole thickens and either flattens or begins to curve outward. When standing, the horse continually shifts its body weight from one foot to the other. X‑rays reveal rotation of the coffin bone, as well as a diseased state in which the bone has become very porous. The top of the bone is forced downward and presses on the sole. In severe cases, it may poke through the sole just in front of the point of the frog.
To diagnose laminitis, a medical history is taken, noting possible contributing factors, such as a grain overload in the diet. The posture of the horse, any abnormalities of the hooves, and a reluctance to move are key parts of the physical examination. Local nerve blocks (regional analgesia) may also be helpful. X-rays are necessary to determine whether the coffin bone is displaced. Mild cases with no visible hoof deformity can be identified by x‑rays of the affected feet.
Treatment and Outlook
Acute laminitis is considered a medical emergency because coffin bone displacement can occur quickly. If laminitis is suspected, your veterinarian should be contacted immediately.
Your veterinarian may prescribe certain nonsteroidal anti-inflammatory medications to lessen inflammation and pain.
Cooling the affected foot by placing it directly in ice water (called digital hypothermia) may protect the laminae early on in horses at risk for developing septic laminitis. Your veterinarian will let you know whether this therapy is appropriate for your horse.
During the first 2 to 3 weeks, it is important to remove standard shoes, because shoes place the majority of stress on the hoof wall and therefore the laminae. The feet and soles should be padded with a soft, resilient substance that is angled to reduce pressure on the front of the hoof. Based on xray changes and when the horse stabilizes, your veterinarian and farrier will advise when and how to shoe the horse again after a bout of acute laminitis.
Treatments of chronic laminitis have attempted to restore the normal alignment of the rotated coffin bone. This requires corrective hoof trimming and shoeing with an appropriate shoe (such as heart-bar shoes, egg bar shoes, natural balance shoes, or Steward clogs).
Surgical options include severing of the deep digital flexor tendon (tenotomy) and removal of a section of the separated hoof wall. Deep digital flexor tenotomy is most commonly performed in cases of chronic rotation that do not respond to shoeing techniques. The application of heel wedges or other techniques is also necessary to stabilize the coffin bone after surgery. Hoof wall resections are performed much less frequently now than in the past. Only a small portion of the hoof wall is removed, because removing larger portions causes severe instability within the hoof.
Despite prompt treatment, the outlook for recovery is guarded until recovery is complete and it is evident that the hoof structure is not altered.
Pedal Osteitis
Pedal osteitis is diagnosed when veterinarians see mineral loss from the coffin bone on x-rays of the foot. This bone loss usually occurs due to longterm or repeated pressure, trauma, or inflammation of the area. Repeated jarring injuries, laminitis, persistent corns, and chronic bruised soles have been implicated as causes. Pedal osteitis is common in performance horses and usually is associated with work on hard tracks.
Because the bone loss is permanent, the presence of pedal osteitis on x-rays does not always indicate a current problem. Your veterinarian will perform a thorough examination. Lameness may not be obvious. There may be a stilted or shuffling action in front, with signs of discomfort in the hoof region. If there is current inflammation, tapping and pressure from hoof testers usually reveal tenderness over the entire sole. Local nerve blocks (regional analgesia) can also help identify the source of the problem. X-rays are helpful in diagnosis and can be used to help differentiate this condition from others with similar signs.
Treatment involves managing the underlying disease. This may include prolonged rest, anti-inflammatory medication, and careful shoeing to relieve sole pressure.
Puncture Wounds of the Foot
Puncture wounds can occur when a horse steps on a penetrating foreign object. Nail bind implies that a nail has been driven close to the sensitive structures of the foot, causing severe pain and lameness. Nail prick means that the thick, sensitive layer of connective tissue beneath the outer layer of skin has been pierced.
When a foreign object penetrates the sole of the foot, it can introduce microorganisms that can cause infection. A pocket of infection and pus (called a subsolar abscess) can readily form. Lameness is usually severe following a puncture wound, especially when the foot bears weight; the degree of lameness may be similar to that produced by a fracture. The horse may stand and point the affected foot. The foot will show increased pain and may be warm to the touch. The infection may progress to the coronary band, which can swell and rupture. Subsequently, the pastern and fetlock areas accumulate fluid and swell. Diagnosis requires confirming the site of pain by pulling the shoe, applying hoof testers, and paring down the suspect area to locate the foreign object or its path of entry.
Puncture wounds in or near the frog often penetrate important structures within the foot, including the navicular bursa, the coffin joint, or the tendon sheath of the deep digital flexor tendon. The resulting infection is very serious and requires rapid diagnosis and treatment. X-rays can help identify which structures are affected.
Prompt treatment with disinfectants and poultices is also important for inadvertent shoeing injuries, when a nail is placed too close to the sensitive layer of the hoof wall. (This is also called “nail bind”, “hot nail”, or a “nail prick”.) Ensuring adequate wound drainage helps prevent the formation of abscesses. In pricked foot, the outlook for recovery is good, provided diagnosis is made and treatment begun early.
Any foreign object must always be found and removed, and the infected area pared with a hoof knife to allow adequate drainage. If an abscess has formed, your veterinarian may also flush the wound every 1 to 2 days for several treatments. The foot should be protected (for example, kept in a rubber or plastic boot) until there is full healing of the puncture site. Healing tends to be much more rapid and is easier to treat if the infection entered through the wall instead of the sole. All horses with puncture wounds should be immunized against tetanus. If the pain is severe, regional analgesia provides temporary relief. Antibiotic treatment is not necessary, provided the infection is localized and good drainage has been achieved. However, antibiotics may be needed if the coronary band is affected. Deep punctures of the foot that involve the deep digital flexor tendon, navicular bursa, navicular bone, or coffin bone require emergency surgery and antibiotics.
Quittor
Quittor is a longterm (chronic) inflammation of the cartilage of the coffin bone characterized by death of the cartilage and one or more sinus tracts extending from the diseased cartilage through the skin. It is seldom encountered today but once was common in working draft horses.
In most cases, injury to the coronet or pastern introduces infection into the deep tissues, forming a pus-filled sore called an abscess. Quittor may also occur after infection enters the foot through a crack in the hoof wall (see below). The first sign is an inflammatory swelling over the cartilage, followed by the formation of draining tracts. During the inflammatory stage, lameness occurs.
Surgery to remove the diseased tissue and cartilage is usually successful. Drug treatment without surgery is likely to fail. Without treatment and drainage the cartilage will die, and abscesses will recur and extend to deep structures, leading to longterm lameness. If damage is extensive and the distal phalangeal (coffin) joint has been invaded, the outlook for recovery is unfavorable.
Sandcrack (Toe Crack, Quarter Crack, Heel Crack)
In sandcrack, cracks in the wall of the hoof begin at the coronet and run down the hoof. It is thought to occur due to excessive pressure placed on the hoof wall and the coronary band. Inappropriate shoeing (such as using a small shoe or a delay in resetting of the shoes) may be to blame.
A crack in the horn coming from the coronet is the most obvious sign of sandcrack. Lameness varies depending on the site and extent of the injury; if infection is involved, lameness may be accompanied by a bloody or pus-filled discharge and signs of inflammation.
Treatment involves trimming and corrective shoeing to change the distribution of weight on the hoof. The use of bar shoes is often recommended. A veterinarian can then remove any diseased tissue from the crack. If the crack has become infected, an antiseptic may be used. The veterinarian may also stabilize the crack with surgical wires, screws, putty, and/or drains. The hoof is then bandaged until new horn formation is evident.
Scratches (Greasy Heel, Dew Poisoning, Pastern Dermatitis)
Scratches, sometimes referred to as greasy heel, is a longterm inflammation of the skin in which the rear surface of the pastern and fetlock enlarge and ooze discharge. It often is associated with poor stable hygiene, but no specific cause is known. Heavy horses (such as draft horses) are particularly susceptible, and the hindlimbs more commonly are affected. Standardbreds often are affected in the spring when tracks are wet.
Scratches may go unnoticed in horses with feathers, because the long, dense hair makes it difficult to see the lesions. The skin is itchy, sensitive, and swollen during the early stages; later, it thickens and loses all but its shorter hairs, which stand in an upright position. The surface of the skin is soft, and the grayish discharge has a rotten odor. If the condition continues longterm, small masses of tissue (called granulomas) may appear. Lameness may or may not be present, but it can be severe if inflamed tissues beneath the skin of the limb become infected. As the condition progresses, the skin of the affected regions thickens and hardens.
Persistent and aggressive treatment is usually successful. This consists of removing the hair, regular washing and cleansing with warm water and soap to remove all soft discharge, drying, and applying an astringent dressing. If granulomas appear, a veterinarian may remove them. Deep infection requires whole-body antibiotics and vaccination against tetanus.
White Line Disease (Seedy Toe, Hollow Wall)
White line disease (seedy toe) involves separation of the hoof wall. The separation probably starts because of abnormal wall stress due to poor foot shape or trimming (for example, a long toe, underrun heels). It can start at the toes, quarters, or heel. Displacement of the coffin bone can occur, similar to laminitis. The outer surface of the wall may appear sound, but a cavity between the hoof wall and the laminae can be seen on the solar surface of the foot. Microorganisms can invade this cavity and cause infections. Tapping on the outside of the wall at the toe produces a hollow sound over the affected portion. Lameness is infrequent but may occur if infection, an abscess, or displacement of the coffin bone is also present.
The condition is diagnosed with a physical examination and x-rays. For treatment, corrective trimming is critical to correct abnormal stresses on the hoof wall. All of the separated hoof wall will likely be removed. Your veterinarian may recommend the use of a topical antiseptic. Corrective shoeing (for example, a heart bar or egg bar shoe) is critical to provide adequate support to the remaining foot and remove stress from the affected areas.
Sheared Heels
In sheared heels, unevenness of the heels produces a severe imbalance of the foot. Hoof cracks, deep cracks between the rounded parts (bulbs) of the heel, and an infection of the frog (thrush) frequently accompany the problem. Sheared heels are most likely caused by abnormal pressure being placed on one side of the foot, usually due to abnormal confirmation of the leg or foot. Navicular disease may occur at the same time.
Heel alignment and foot balance may be restored with corrective trimming and shoeing. A full bar shoe with a reinforcing diagonal bar to support the affected quarter and heel is used. Improvement will likely require several shoe resettings. The outlook for recovery is good in uncomplicated cases, if corrective measures are consistently applied until new hoof growth occurs.
Sidebone
Sidebone is the hardening (calcification) of the cartilage of the coffin bone. It is most common in the forefeet of heavy horses working on hard surfaces. It also is frequent in hunters and jumpers but is rare in racing Thoroughbreds. Repeated jarring injuries to the quarters of the feet are probably the most basic cause. Improper shoeing that stops normal movement of the quarters may also lead to sidebone. Other cases arise from direct trauma.
Sidebone rarely causes lameness and is generally an incidental finding (ie, found by accident) on xrays taken of the foot for another reason.
Thrush
Thrush is a degeneration of the frog with secondary bacterial infection. Although some people blame poor management and hygiene as its cause, it is more likely caused by poor conformation or trimming of the foot and a lack of exercise. Exercise may help clean out the hoof when the weight of the horse pushes down on the frog and surrounding structures. Thrush also occurs in horses with sheared heels (see above). The condition is more common in the hind feet. The affected area is moist and contains a black, thick discharge with a characteristic foul odor, and tissue at the borders of the frog may be dead. These signs alone are sufficient to make the diagnosis.
Treatment should begin by providing dry, clean material underfoot and cleaning out the hoof, including the removal of all softened horn. An astringent lotion, used with daily hoof cleaning, aids recovery after removal of the diseased tissue. Additionally, the foot needs to be balanced, with affected horses placed on a regular exercise schedule in a dry area. Use of a bar shoe after the disease has been stopped may help the frog regenerate. Although it may not cause the condition, a moist environment should be avoided in animals with thrush. The outlook for recovery is usually favorable with appropriate changes in shoeing and exercise.





