

Various problems related to calcium, including hypocalcemia, sudden death, osteoporosis, and cage layer fatigue, have been observed in hens.
Pullets or hens with insufficient dietary calcium, phosphorus, or vitamin D3 may die suddenly or be found paralyzed from hypocalcemia while shelling an egg. This may be associated with high production and withdrawal of calcium from bones for eggshell production, in which case the main lesion may be osteoporosis.
At necropsy, there is an egg in the shell gland and the ova are active and fully developed. There are no other lesions, although medullary bone may be lacking. Paralyzed hens respond to calcium IV, and this response may be useful in diagnosis.
Osteoporosis is a major cause of death in high-production flocks. Hens with osteoporosis may show similar signs at necropsy, or the ova may be regressing with no egg in the oviduct. The femur is always fragile and medullary bone is always absent in osteoporosis.
Affected hens may also respond to intravenous administration of calcium if there are no fractures of the legs or vertebrae. The use of large particle size calcium (limestone, oyster shell) in the diet may be beneficial.
High rates of mortality due to fractures are common in birds affected with osteoporosis. This situation is more common in broiler breeder hens in slatted houses due to the trauma caused by jumping on and off the slats. Ruptured egg follicles indicating trauma can be found at necropsy.
Hypocalcemia, or calcium tetany (paralysis), occurs in modern or high-yielding broiler breeder hens. This syndrome is characterized by an acute and sudden onset, usually in flocks with good hen-day production.
Clinical signs such as panting, spread wings, and prostration may be evident in the early morning hours preceding paralysis and death. Hens may be down in the scratch, unable to rise. They become paralyzed and are the object of increased mating attempts and male aggression (often misdiagnosed as male kills; see ).


Paralyzed, panting hen affected by hypocalcemia.
Courtesy of Dr. Rodrigo Espinosa.
Careful postmortem examination reveals a fully active ovary (8–9 large yellow follicles), the presence of a partially or fully formed egg in the shell gland, and signs of asphyxia, such as a cyanotic comb, congested lungs, and dark musculature (see ). This indicates that the hen used all available calcium from the bloodstream in an effort to complete the eggshell.
The condition is common in flocks with poor body weight uniformity that are fed diets with a high calcium concentration (> 1.2%) in the weeks before the onset of lay and brought into production by drastic increases in day length and feed allocation.


Partially formed egg in the reproductive tract of a hen affected by calcium tetany. Note the overstimulated and congested ovary.
Courtesy of Dr. Rodrigo Espinosa.
Less common causes of hypocalcemia are low calcium concentrations in breeder feed, too-small limestone particle size, and exaggerated separation of heavy minerals in mash feed.
This condition seems to be more common during the hot weather months, and it can be exacerbated by inadequate cooling and ventilation:
Heat stress triggers gular flutter—effectively panting or hyperventilation—as a means to cool and dissipate heat in avian species.
Hyperventilation decreases the partial pressure of CO2 in circulating blood and thus increases in blood pH, which is conversely associated with decreased blood concentrations of ionized calcium (the form of calcium required for normal muscle function and nerve transmission).
Decreased ionized calcium, particularly in a bird in which calcium metabolism may already be compromised, can precipitate the onset of calcium tetany.


Bulked pectoral muscle in a hen from a parent stock flock affected by sudden death syndrome.
Courtesy of Dr. Rodrigo Espinosa.
Cases are often reported in the early morning after feeding, a time when birds in a commercial setting intentionally gather together in a smaller space to consume feed, decreasing the ability of moving air to effectively cool birds and increasing metabolic heat production.

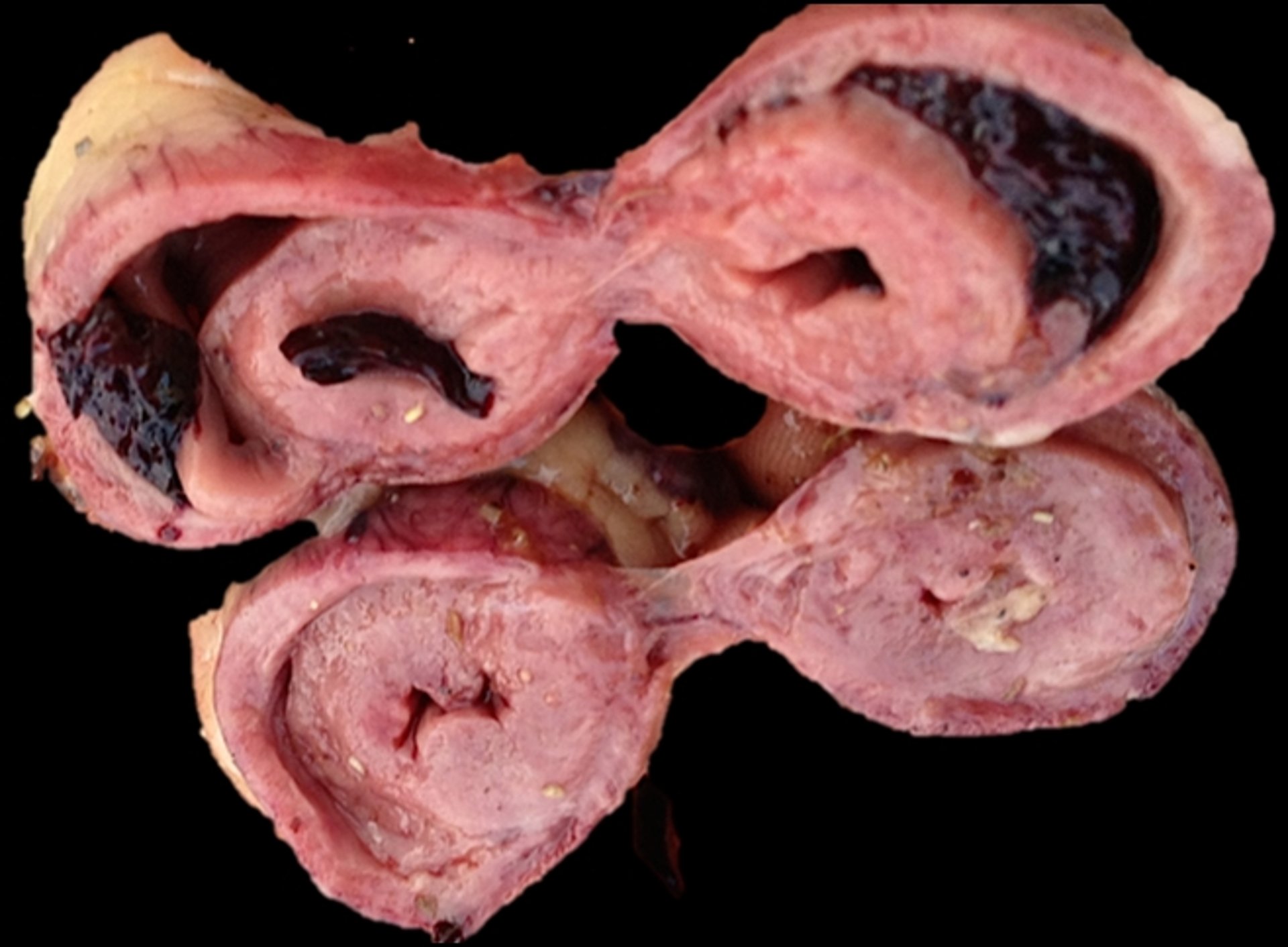
Enlarged left side of heart and dilated right of heart in a hen from a parent stock flock affected by sudden death syndrome.
Courtesy of Dr. Rodrigo Espinosa.
Hypocalcemia can be prevented by management practices that promote body weight uniformity and avoid excessive or premature allocation of high-calcium diets and light stimulation.
Mortality rates can be decreased by the administration (“topping of the feed”) of 5 g of oyster shell per hen for 3 consecutive days and the addition of vitamin D3 to the drinking water. This treatment should be suspended for 3 days and then repeated. Severe cases will require continual treatment for 2–3 weeks (3 days of treatment followed by 3 days without).
Overtreatment can be harmful.
Feeding recommended levels of calcium, using large particle size calcium, and providing adequate ventilation and cooling are helpful to prevent or decrease the incidence of this condition.
Death and the presence of an egg in the shell gland also can be caused by a condition referred to as sudden death syndrome, first reported in Australia (see ).
Sudden death syndrome has been associated with refeeding syndrome (see ).
Immature and undersized pullets that have been fed too much too fast could develop sudden death if the feeding program provides higher nutrients than their requirements.
The following are typical in affected birds:
bulked pectoral muscles
juvenile ovarian development
generalized internal congestion
hydropericardium
enlargement of the left side of the heart
dilated right side
Often, sudden death syndrome is confused with calcium tetany. Some trigger factors are feed rations low in phosphorus, potassium, protein, and energy but rich in calcium, resulting in cardiomyopathy.





