

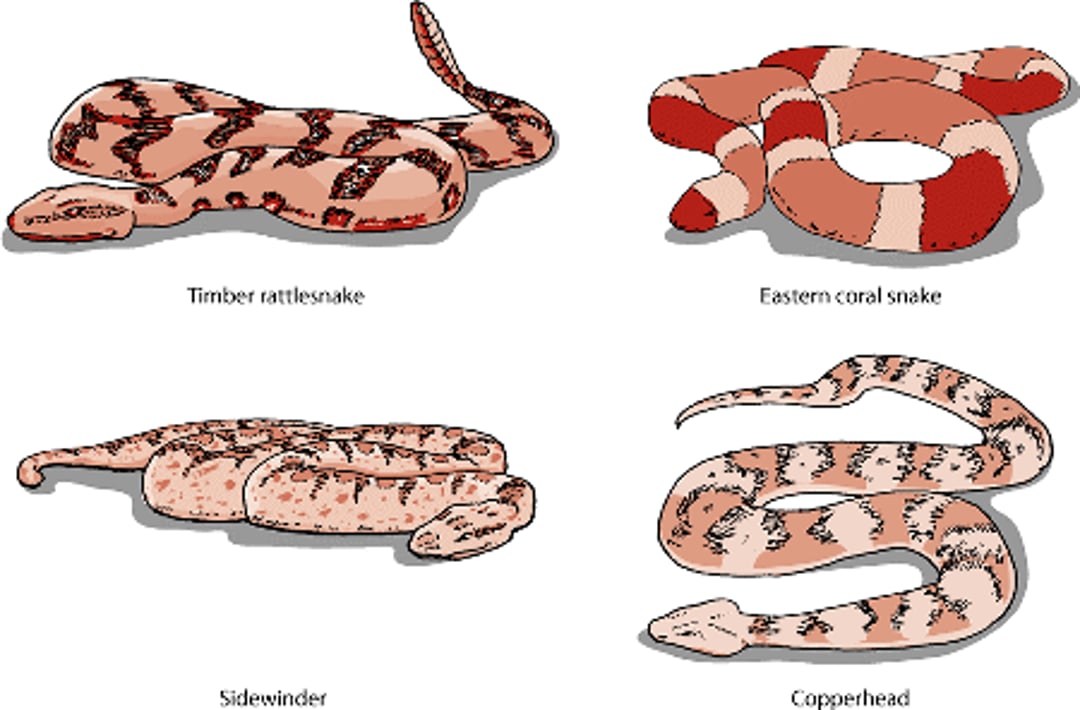
Venomous snakes fall into two families: 1) the Elapidae, which include the cobra, mamba, and coral snakes; and 2) the Cortalidae, which include the true vipers (for example, puff adder, Russell’s viper, and the common European adder) and the pit vipers (for example, rattlesnakes, cottonmouth moccasin, copperhead, and fer-de-lance). Pit vipers and coral snakes are found in North America.
Elapid snakes have short fangs and tend to hang on and “chew” venom into their victims. Elapid venom is toxic to the nervous system and paralyzes the breathing center. Animals that survive these bites generally recover completely. Crotalid snakes have long, hinged, hollow fangs; they strike, inject venom, and withdraw. Crotalid venom is typically toxic to the blood, killing cells and preventing normal clotting. The venom of some crotalid species, for example, the Mojave rattlesnake, also affects the nervous system.
Poisonous snakes

Deadly snakebites are more common in dogs than in any other domestic animal. Because many dogs are relatively small in size in proportion to the amount of venom injected, the bite of even a small snake can be fatal. Due to their large size, horses seldom die as a direct result of a snakebite, but bites on the muzzle, head, or neck that cause swelling and difficulty breathing can lead to death. Secondary damage can be serious; for example, a bite near the coronary band may cause a hoof to die and fall off.
A venomous snakebite is a true emergency. Rapid examination and appropriate treatment by a veterinarian are paramount. Owners should not spend time on first aid other than to keep the animal quiet and limit its activity.
In many instances, someone has witnessed the bite. Other conditions that are sometimes mistaken for snakebite include fractures, abscesses, spider bites, or allergic reactions to insect bites or stings. When possible, owners should bring the dead snake along with the bitten animal. The snake’s head should not be damaged because identification often depends on the type of head.
Many bites do not result in venom being injected, or are made by nonpoisonous snakes. Typical pit viper bites are characterized by severe local tissue damage that spreads from the bite site. The tissue becomes discolored within a few minutes, and dark, bloody fluid may ooze from the fang wounds if not prevented by swelling. Often the outer layer of the skin separates when the overlying hair is clipped or merely parted. Hair may hide the fang marks. Sometimes, only one fang mark or multiple punctures are present. In Elapid snakebites, pain and swelling are usually minimal.
Intensive treatment should be started as soon as possible because irreversible effects of venom begin immediately after the bite. Animals bitten by an Elapid snake can be treated with antivenin (which may be available through human hospital emergency rooms) and supportive care. Antivenin against North American pit vipers is available and should be used for all pit viper bites.
After injection of venom by a pit viper, signs are divided into three phases: the first 2 hours, the next 24 hours, and a variable period (usually about 10 days) afterward. In the first 2 hours, untreated animals usually die. If the animal is active and alert after 24 hours, death due to the direct effects of the venom is unlikely. The third phase is a recovery period, but infection can cause extensive cell damage, leading to tissue death that may involve an entire limb.
In dogs and cats, death rates are generally higher from bites to the chest or abdomen than from bites to the head or extremities. However, this may relate to the size and vulnerability of the victim, because smaller animals are more likely to be bitten on the body.
A bite during which a snake injects venom is a true emergency. Rapid examination and appropriate treatment are paramount. Owners should not spend time on first aid other than to keep the animal quiet and limit its activity. The following commonly touted measures are ineffective and can be potentially harmful: use of ice, cold packs, or sprays; incision and suction; tourniquets; electric shock; hot packs; and delay in presentation for medical treatment (waiting until problems develop).
Treatment for a pit viper bite includes treating for shock, neutralizing the venom, controlling blood clotting, and preventing secondary infection. Antivenin is highly beneficial because its action is the only direct and specific mechanism for neutralizing snake venom. Antivenin treatment is most effective if given within 6 hours of the bite. Antibiotic treatment should continue until all superficial tissue changes have healed. Tetanus antitoxin also should be given. In most cases, attempting to surgically remove the wound is impractical or unwarranted. There is also a vaccine available for dogs that may reduce the effects of a rattlesnake bite.
Animals bitten by coral snakes or other elapids may be treated with supportive care as needed and antivenom, if available. Animals bitten by Australian elapid snakes may need to be placed on a ventilator to support breathing. Coral snake antivenom is no longer being manufactured in the US, although some practitioners have received special permission to import it from Mexico. In Australia, several antivenoms/antivenins are available for use in veterinary patients. An antivenin effective against multiple types of snakes is available for use when the snake cannot be identified, and many clinicians prefer to use the polyvalent antivenin for all envenomations. Additionally, animals bitten by Australian elapids should be monitored for development of bleeding problems and kidney, heart, or muscle damage. As with crotalid bites, antibiotics may be given if there is risk of infection of the bite wound.
For More Information
Also see professional health content regarding snakebites to animals.





