

Triage is the method of assigning priority to emergency patients and their problems based on rapid assessment of historical and physical parameters (see the table ).
Several historical or observed problems warrant transferring the animal to the treatment area regardless of physical findings. All members of the veterinary medical staff should be able to recognize these common complaints so that immediate (stat) evaluation by a veterinarian can occur; these conditions can require rapid intervention or lead to rapid decompensation:
allergic reaction, particularly if there is evidence of shock or airway obstruction
bleeding
cardiopulmonary arrest
collapse, immobility, inability to walk, loss of consciousness, or severe alteration in mental state
difficulty urinating or inability to urinate in male cats
heatstroke
hypothermia
paleness, weakness (anemia; see images of and
profuse vomiting
profuse diarrhea
prolapsed or eviscerated organs
respiratory difficulty
seizures
substantial pain
snakebite
swollen or painful abdomen or nonproductive retching (gastric dilation and volvulus)
toxin ingestion
trauma or open wounds
Parameters to Evaluate During Triage
Parameter | Evaluation | Significance |
|---|---|---|
Mucous membrane color | Pink | Normal PCV and adequate perfusion |
Pale or white | Anemia or shock | |
Cyanotic or muddy | Severe hypoxemia or decompensatory shock | |
Yellow | Increased serum bilirubin due to hepatic disease or hemolysis | |
Local or systemic disease | Focal changes to mucous membranes, such as petechia or redness, swelling, sloughing of superficial layers, or very dark or black discoloration; can also indicate systemic disease. | Petechia may indicate thrombocytopenia or thrombocytopathy; redness and swelling or sloughing may indicate local chemical, thermal, or electrical injury; dark or black discoloration may indicate loss of blood supply with thrombosis, necrosis, etc. |
Capillary refill time | 1–2 seconds | Normal perfusion and rapidity with which capillaries refill with blood |
> 2 seconds | Poor perfusion or peripheral vasoconstriction | |
< 1 second | Hyperdynamic state; could be associated with fever, heatstroke, distributive shock, or early compensatory stage of hypovolemic shock | |
Heart rate | 70–120 bpm (small dogs) 60–120 bpm (large dogs) 150–220 bpm (cats) | Normal heart rates; indicate that at least one component of cardiac output is normal |
Bradycardia: < 60–70 bpm (dogs) < 150 bpm (cats) | Decreased cardiac output and subsequent poor perfusion; cats in particular develop bradycardia (< 120 bpm) in shock; an irregular, slow heartbeat can be associated with imminent cardiac arrest, severe arrhythmias, or metabolic derangements (hyperkalemia, hypocalcemia, etc) | |
Tachycardia: > 180 bpm (dogs) > 220 bpm (cats) | Compromised diastolic filling; sinus tachycardia often results from hypovolemic shock, pain, or primary cardiac disease; tachycardia that is irregular or associated with pulse deficits usually indicates an arrhythmia, and an ECG is indicated | |
Pulse rate and quality | Strong and synchronous with each heartbeat | Normal; both femoral and digital pulses should be palpated |
Irregular | Usually indicative of a cardiac arrhythmia | |
Bounding | Hyperdynamic (compensatory) state of shock; indicates an increase in pulse pressure (ie, an increase in systolic pressure, decrease in diastolic pressure, or both) | |
Weak or absent | Decreased cardiac output (including cardiopulmonary arrest), peripheral vasoconstriction, decreased pulse pressure, or thrombosis | |
Level of consciousness | Alert and responsive to surroundings | Normal overall neurological and metabolic state |
Depressed or obtunded (less responsive to visual and tactile stimuli, sleepy appearance but still arousable) | Can be caused by any illness or decreased perfusion; may be mild, moderate, or severe | |
Stupor (arousable only with painful stimuli) | Severe neurological or metabolic derangements, including toxin ingestion | |
Comatose (unarousable with any stimuli) or seizures (usually associated with whole body seizures, salivation, facial tremors, possibly involuntary urination and defecation) | Abnormal cerebral electrical activity from primary neurological disease or secondary to metabolic derangements in diseases such as diabetes mellitus, hepatic encephalopathy, hypoglycemia, or toxin exposure; accurate history or prior health problems, current medications, and possible toxin exposure important | |
Level of pain | Vocalization, changes in behavior (avoidance, aggression), or physical changes (tachycardia, dilated pupils, etc). This is best recorded with a composite pain scale. | Clinical signs can be similar to those of compensatory stage of shock; pain delays healing and must be treated. |
In triage of an animal undergoing evaluation on an emergency basis, a primary survey (a rapid assessment) is performed to assess patient stability and identify problems so that immediate treatment can be initiated. After the primary survey and initial stabilization are complete, a secondary survey (a thorough examination) is performed. This chapter cannot address all emergency presentations; for specific problems, the reader is referred to additional chapters and For More Information.
The traditional primary survey has focused on life-threatening problems; the ABC approach (for airway, breathing, circulation) is a systematic method for prioritizing and treating life-threatening emergencies. The Veterinary Committee on Trauma (VetCOT) supports updating the primary survey for trauma patients to XABCDE (for eXsanguination, airway, breathing, circulation, disability, and exposure), to particularly prioritize the importance of arresting hemorrhage. Hemorrhage can be a major cause of mortality in bleeding patients (which can apply to trauma, but also to internal hemorrhage, such as with a hemoabdomen from ruptured neoplasia or coagulopathy); the expanded primary survey also addresses neurological injury and open wounds. (See .)


Note that the updated primary survey prioritizes arresting hemorrhage and adds steps evaluating disability and exposure.
Courtesy of the Veterinary Committee on Trauma, American College of Veterinary Emergency and Critical Care, and Colorado State University.
Because the ABC approach can be applied to all patients presenting to the ER, these elements will be covered thoroughly, and the other components briefly discussed for completeness. Each area of focus—XABCDE—should be sequentially evaluated and addressed:
X (eXsanguination): obvious catastrophic external or internal cavitary hemorrhage
A (airway): ensuring the patient's airway is clear and open
B (breathing): assessing the patient's respiratory rate and effort, as well as oxygenation status
C (circulation): auscultating the heart and assessing for clinical signs of adequate blood flow, such as heart rate, pulse quality, mucous membrane color, capillary refill time [CRT], and blood pressure
D (disability): evidence of head or spinal injury or disease, examining the central and peripheral nervous system
E (exposure risk/environment): changes in body temperature, sources of heat loss and open wounds
Finally, many emergency conditions can be painful, and this should also be addressed.
Problems within the categories of hemorrhage, airway, breathing, and circulation can be reasons for an animal to be in catastrophic distress and include the following:
eXsanguination: trauma, ruptured neoplasia, coagulopathies, organ failure
Airway: airway obstruction or disruption
Breathing: problems from pleural space or chest wall disease (air, especially tension pneumothorax or various intrapleural fluids), alveolar flooding (edema, blood, or inflammatory fluid), severe bronchoconstriction with air trapping, and brainstem lesions or severe metabolic or electrolyte abnormalities affecting oxygenation and ventilation
Circulation: shock (decreased perfusion of any etiology: hypovolemic or hemorrhagic, distributive, cardiogenic or obstructive; see the chapter Fluid Therapy), cardiopulmonary arrest
The final two primary survey components, disability and exposure/environment, are not problems in all emergency patients but should receive particular attention in patients with neurological injury (D) and trauma patients (D and E):
Disability: evaluation of injury to or disease of the central (brain and cranial nerves) or peripheral (spinal cord and peripheral nerves) nervous system; these injuries can have devastating consequences if they are severe and not addressed quickly.
Exposure/Environment: assessing the patient's body temperature and potential sources of heat loss, including open wounds
Pain management, assessing and appropriately addressing painful conditions, is also essential for the emergency patient.


Very pale to white mucous membranes in an anemic cat.
Courtesy of Dr. Andrew Linklater.


Normal pink mucous membranes in an anesthetized dog.
Courtesy of Dr. Andrew Linklater.
Bleeding Disorders in Small Animal Emergency Patients
Diagnosis of Hemorrhage in Animal Emergency Patients
External hemorrhage is usually easy to identify; however, internal hemorrhage can be more challenging. Animals with hemorrhage greater than class I exhibit clinical signs of shock; however, the volume of blood lost prior to arrival at the hospital is often unknown for ER patients. Any blood lost at the hospital should be quantified or estimated. This can be easily achieved when the blood is collected in a closed system; gauze or other absorptive material should be weighed to estimate the amount of blood loss.
There are four classes of hemorrhage:
Class I hemorrhage (minimal): < 15% of blood volume lost (< 13 mL/kg dog, < 9 mL/kg cat). This amount of blood loss is usually associated with minimal clinical signs (tachycardia or rapid CRT) and may resolve without intervention.
Class II hemorrhage (mild): 15–30% of blood volume lost (13–26 mL/kg dog, 9–18 mL/kg cat). This results in clinical signs such as tachycardia, alternations in pulse quality (bounding) and blood pressure, and rapid CRT; these patients usually require resuscitation.
Class III hemorrhage (moderate): 30–40% of blood volume lost (26–35 mL/kg dog, 18–24 mL/kg cat). This results in severe clinical signs, which may include hypotension and tachycardia; these patients usually require resuscitation with blood products.
Class IV hemorrhage (severe): ≥ 40% of blood volume lost (≥ 35 mL/kg dog, ≥ 24 mL/kg cat). This results in a patient near death, requiring immediate resuscitation with blood and often surgery to survive.
Hemostasis in Animal Emergency Patients with Hemorrhage
Hemorrhage most commonly occurs in veterinary patients due to trauma, ruptured neoplasia, or coagulopathies (such as anticoagulant rodenticides); however, other causes include liver failure, vessel aneurysms, GI ulceration, and invasive procedures, such as biopsies or surgery. Control of ongoing hemorrhage is essential for stabilization and is often required before or concurrently with restoration of circulation (fluid resuscitation). Achieving normal (or elevated) blood pressure during resuscitation may exacerbate hemorrhage, so conservative end points are recommended.
The patient must be carefully and thoroughly examined for any evidence of external hemorrhage. Direct pressure should be immediately placed over any bleeding site, and bleeding arteries and veins should be clamped and/or ligated. Occasionally, cautery devices may be used to assist with hemorrhage; however, these can be painful, and the patient may need to be sedated. If blood is slowly oozing from a wound, a compression bandage should be placed. Topical hemostatic agents such as kaolin- or chitin-impregnated gauze material may be applied to wounds. Deep, bleeding wounds can be tightly packed with gauze material to help arrest hemorrhage (see ).


A dog that has sustained trauma and is experiencing substantial hemorrhage from a left forelimb injury. In this situation, immediate measures must be taken to control hemorrhage with compression, packing, cautery, bandaging, ligation, or tourniquet.
Courtesy of Dr. Andrew Linklater.
With limb or tail hemorrhage, a blood pressure (pneumatic) cuff or tourniquet can be temporarily placed until coagulation occurs or surgical intervention is used to stop bleeding. Tourniquets should not remain in place for > 10 minutes, as they compromise normal blood flow required for healing.
Nasal or oral hemorrhage may require sedation and intubation. Topical epinephrine may be applied; however, if hemorrhage is substantial, it is likely to be rapidly diluted and ineffective. Packing the nares and caudal oropharynx is often sufficient to stop substantial nasal hemorrhage (see and images).

Substantial nasal hemorrhage in a dog.
Courtesy of Dr. Andrew Linklater.

A patient is anesthetized and intubated to control nasal hemorrhage. The nares have been packed tightly with cotton-tipped applicators, left in place for 10–15 minutes. Not pictured is the caudal oropharynx, also tightly packed with rolled gauze. Rolled gauze is used so it can be easily retrieved.
Courtesy of Dr. Andrew Linklater.
Intrathoracic or abdominal hemorrhage may be difficult to detect on physical examination and may be exacerbated when blood pressure and circulation are restored.
Abdominal, thoracic, and cardiac point-of-care ultrasound (APOCUS, TPOCUS, CPOCUS) techniques can be used to rapidly identify free abdominal, thoracic, or pericardial fluid; however, retroperitoneal and pelvic hemorrhage can be more challenging to identify:
In the abdomen, the probe is focused on the ventral midline caudal to the xiphoid, over the urinary bladder, and on the right and left dependent flank regions.
For the thorax, the probe is used to examine a minimum of four points of each hemithorax; however, any region may be examined.
The cardiac window is used on the right and left sides (ribs 3-5, cranioventrally) to examine the heart.
A four-quadrant abdominocentesis can be performed if ultrasonography is not immediately available.
PCV of thoracic or abdominal fluid within 5–10% of the PCV of peripheral blood or PCV > 25% confirms hemorrhage. Sizable volumes of cavitary hemorrhage can be collected into sterile collection systems (such as an empty IV bag or blood transfusion bag) for autologous blood transfusion (ABT), because available allogenic blood for transfusion is often a limiting resource in veterinary hospitals (see ).

This patient is experiencing substantial abdominal hemorrhage. The blood is being aseptically collected from the abdomen in a closed system and then delivered IV through a filter.
Courtesy of Dr. Andrew Linklater.
In patients with ongoing hemorrhage, the lethal triad of acidosis, hypothermia, and hypocoagulation must be recognized and addressed. Each is a contributing factor to the other and may result in death of the patient, so arresting the hemorrhage and resuscitating with fluid (or blood) must occur quickly. With abdominal hemorrhage, lack of response or resolution and return of shock likely indicate surgical intervention is necessary.
Although making the patient as stable as possible is best, rapid and aggressive surgical intervention may be required. Free blood should be collected in a sterile canister for possible autologous blood transfusion. In surgery, the abdominal cavity is then packed off and explored quadrant by quadrant to identify the source of hemorrhage. With ruptured neoplasia, organ or mass removal is often necessary; with trauma, organ removal may be necessary. With crush injury (common to the liver and spleen), organ removal may be impossible, however, in such cases, damage control techniques are instituted.
Damage control resuscitation has been associated with improved outcome in human trauma patients and has several guiding principles:
permissive hypotension to avoid exacerbation of hemorrhage using small-volume fluid resuscitation to low-normal end points
the early use of blood products (transfusion) for resuscitation
minimizing a large volume of crystalloids during resuscitation
correcting acidosis, hypothermia, and coagulopathy
immediate hemorrhage control
Hemorrhage control may be through medical means (such as administration of antifibrinolytics or plasma, when indicated) along with surgical means.
Damage control surgery is a limited abdominal procedure with minimal anesthesia time to arrest hemorrhage by using intra-abdominal packing and to minimize further contamination without definitive surgical exploration; definitive care is delayed until the patient is stable. This is an uncommon technique in veterinary medicine.
When abdominal surgery is not possible or needs to be delayed, abdominal and hindlimb counterpressure (see below) may be used.
Ongoing intrathoracic hemorrhage should be managed with thoracocentesis or a thoracostomy tube to evacuate blood and to allow measurement of the volume lost. Exploration of the thorax may be required for definitive hemostasis.
Hindlimb and Abdominal Binding in Animal Emergency Patients
When ongoing abdominal hemorrhage is suspected from trauma, hindlimb and abdominal counterpressure can improve perfusion (see ). This procedure compresses the arteries and arterioles within the bound regions, increasing regional vascular resistance and producing abdominal tamponade, thereby effectively slowing or arresting hemorrhage and redirecting blood flow from the venous capacitance vessels in the caudal half of the body to the more central (core) circulation. The procedure may be used when surgery must be delayed or is not possible.

Abdominal and hindlimb counterpressure placed in a dog with a hemoabdomen secondary to vehicular trauma.
Courtesy of Dr. Andrew Linklater.
Hindlimb and abdominal counterpressure can be performed by first placing a small rolled towel or rolled cotton between the hindlimbs and along the ventral midline of the abdomen. This prevents the wrap from impairing ventilation or fracturing the spleen or liver. If time permits, a urinary catheter should be placed. The hindlimbs and abdomen should then be firmly wrapped with padded bandage material or towels, beginning at the toes of the hindlimb and moving cranially toward the xiphoid, taking care not to impede respiration. The bandage should be secured with tape or nonstretch bandage material wrapped in a spiral pattern, starting caudally and moving cranially.
Abdominal binding should be avoided in cases of intrathoracic or intracranial hemorrhage.
Once perfusion has stabilized for 4–8 hours, the wrap is removed slowly by sections (releasing one section every 15 minutes), starting at the most cranial portion and moving caudally. Any clinical signs of decompensation warrant rapid rebinding of the region last unwrapped.
If the patient is going to surgery, unwrapping, aseptic preparation, and entry into the abdomen must occur quickly.
Patients may also hemorrhage from coagulopathies, which should be ruled out and treated, particularly prior to performing invasive procedures, such as surgery. Centesis, particularly of the pleural or pericardial space, should not be delayed, because these can be not only diagnostic but also lifesaving procedures. Coagulation disorders are most often identified with routine laboratory tests, such as platelet counts (machine count and manual evaluation of a blood smear), or by coagulation times: partial thromboplastin time (PTT), prothrombin time (PT), or viscoelastic testing (see and tracings and tracing).
Thrombocytopenia may be treated with platelet or whole blood transfusions and vincristine (0.02 mg/kg or a maximum of 0.5 mg/m2, IV, once) (1). Coagulation disorders with prolonged PT and PTT are often treated with plasma (eg, fresh frozen plasma, 10–20 mL/kg, IV as needed) or whole blood transfusions to restore normal coagulation times (2). Anticoagulant rodenticide intoxication is also treated with vitamin K1. Viscoelastic testing may indicate hypocoagulation or hyperfibrinolysis (rapid clot breakdown), which can be treated with epsilon aminocaproic acid (50–100 mg/kg, slow IV) (3, 4) or tranexamicacid (10–15 mg/kg, slow IV) (5, 6). Other treatments include antivenin for snakebite and desmopressin (1–4 mcg/kg, IV or SC) for von Willebrand disease (7, 8). Yunnan Baiyao has been anecdotally recommended for bleeding disorders.


This tracing depicts hyperfibrinolysis or rapid clot breakdown. Note the branches of the tracing that narrow towards the right along with the abnormal tracing parameters.
Courtesy of Dr. Andrew Linklater.

This tracing depicts hypocoagulation; note the narrow branches of the tracing along with the abnormal tracing parameters.
Courtesy of Dr. Andrew Linklater.

For comparison with other examples, this is a normal veterinary coagulation monitor tracing.
Courtesy of Dr. Andrew Linklater.
Airway Disorders in Animal Emergency Patients
Airway disorders involving complete large airway obstruction or partial obstruction of the large or small airways can be life-threatening.
Diagnosis of Airway Disorders
Look at the patient and palpate the airway
Listen for abnormal respiratory sounds
Clinical evaluation and intervention must occur rapidly for a patient with airway disease. Evaluation with pulse oximetry may be indicated but should not delay care.
Animals with complete large airway obstruction are unconscious and apneic and require immediate CPR and tracheal intubation (see Treatment of Airway Disorders). During the process of intubation, pulling out the tongue and visually inspecting the pharyngeal tissues and arytenoids can help identify a possible cause of upper airway obstruction.
Partial large airway obstruction causes noisy breathing (stridor or stertor), heard without the aid of a stethoscope. The patient is often cyanotic and anxious; loud referred airway sounds can be heard throughout the thorax on auscultation (see ).


Cyanotic (purple or muddy)-appearing tongue in a dog with partial airway obstruction.
Courtesy of Dr. Andrew Linklater.
Compromise of the extrathoracic airway (nasal passages, pharynx, larynx, or cervical trachea) causes inspiratory stridor, whereas compromise of the intrathoracic trachea or bronchi causes expiratory stridor.
Stertor is most common with pharyngeal disease.
Pathological conditions that may cause large airway obstruction include the following:
foreign body
edema or hemorrhage
laryngeal paralysis/paresis
tracheal collapse or obstruction, including trauma
brachycephalic obstructive airway syndrome (elongated soft palate, stenotic nares, hypoplastic trachea, and everted laryngeal saccules)
aspiration of saliva or stomach contents
neoplasia of any portion of the upper respiratory system or surrounding tissues
Animals with severe small airway obstruction are often anxious and have labored breathing with an expiratory push of the diaphragm. Auscultation reveals high-pitched wheezes throughout the lung field.
In life-threatening cases, the animal may be cyanotic, open-mouth breathing, orthopneic, collapsed, or asphyxiating.
Common causes of small airway obstruction include the following:
bronchial obstruction (from edema, mucus, exudates, inflammatory conditions, or foreign material)
Treatment of Airway Disorders
Reestablish air flow
Deliver oxygen
Establishment of an Airway in Complete Airway Obstruction
Unconscious, apneic animals require immediate tracheal intubation. CPR should be initiated according to the Reassessment Campaign on Veterinary Resuscitation (RECOVER) guidelines, starting with chest compressions at 100–120 bpm, and mouth-to-nose breaths or breaths administered using a tight-fitting mask should be performed until endotracheal intubation is performed at 10 breaths per minute. If only one rescuer is present, a 30 compressions:2 breaths ratio should be performed.
Clinicians should be practiced in orotracheal intubation of animals in dorsal, lateral, and sternal recumbency (see ).

Intubation for substantial laryngeal edema in a brachycephalic dog. Because of the laryngeal swelling, the endotracheal tube is smaller than would typically be used.
Courtesy of Dr. Andrew Linklater.
If an obstruction is present, it must be immediately relieved (with suction, manual removal, the Heimlich maneuver, or external extraction technique [J stroke]) or bypassed via emergency tracheotomy.
Once a patent airway is established, confirmed, and secured, ventilation is initiated with 100% oxygen via a bag valve mask. If auscultation during ventilation detects absent or muffled lung sounds indicative of pleural fluid or air, immediate thoracocentesis is warranted.
Next, heart sounds and pulses are checked, and if absent, CPR is initiated.
Treatment for Partial Large Airway Obstruction
With partial large airway obstruction, flow-by oxygen is delivered through oxygen tubing at a high flow rate aimed at the open, panting mouth until an airway is secured or, if appropriate, a transtracheal or nasotracheal oxygen line is placed (see ).
Heavy sedation using a narcotic or tranquilizer (eg, butorphanol 0.2–0.4 mg/kg, SC, IM, or IV, with or without acepromazine 0.01–0.05 mg/kg, SC, IM, or slow IV) may be used to relieve anxiety in a patient with partial large airway obstruction (such as laryngeal paralysis or brachycephalic airway syndrome). Care must be taken in these patients when using medications such as acepromazine that can cause cardiac or respiratory depression.


Lateral radiograph showing oxygen supplementation administered via nasotracheal oxygen catheter to a dog with tracheal collapse resulting in upper airway obstruction. Note the tip of the catheter ending in the trachea, just past the 3rd rib.
Courtesy of Dr. Andrew Linklater.
When tracheal intubation is necessary, unless the patient is unconscious, general anesthesia should be induced using rapid-acting IV anesthetics. Options for IV medications for rapid sequence induction of anesthesia and intubation include the following:
etomidate (0.5–2 mg/kg)
ketamine (2–10 mg/kg) in combination with a benzodiazepine (ie, diazepam or midazolam at 0.1–0.5 mg/kg)
propofol (2–6 mg/kg, slowly to effect)
alfaxolone (1–3 mg/kg)
Clinicians should choose medications that they are familiar with.
During or immediately before intubation, the ability of the laryngeal cartilages to abduct during inspiration should be assessed and a full oropharyngeal examination performed when time allows.
A tracheotomy is indicated when pharyngeal, laryngeal, or tracheal pathology prevents orotracheal intubation (or when intubation is anticipated to be protracted). A transtracheal catheter can be used to provide oxygen support during stabilization, or the patient can be connected to an anesthetic machine.
Pearls & Pitfalls
|

When the airway pathology lies within the thoracic cavity, airway patency must be established down to the tracheal bifurcation. Once the airway is established, the oxygen tubing should be secured with a tie and the cuff mechanism inflated to the minimum pressure necessary to prevent gas leakage during positive breaths without damaging the trachea, often, a maximum of 20 cm H2O.
Once the airway is secured, intubation should be confirmed with at least two of the following methods:
palpation of the tube within the trachea (only one "tube" palpated in cervical region)
bilateral auscultation of the lungs with a positive pressure breath (with esophageal intubation, gurgling from air/liquid interface in the GI space would be expected)
visualization of chest wall movement with manual ventilation, requiring that the cuff be inflated appropriately
visualization of the tube entering the airway
placement of end-tidal CO2 monitor (normal is 35–45 mm Hg)
thoracic or cervical radiographs
Placement of end-tidal CO2 monitor is the most accurate way to ensure endotracheal intubation. With esophageal intubation, a reading < 5 mm Hg is likely.
Therapy for Small Airway Obstructive Disease
Cyanosis from small airway obstructive disease is treated by providing oxygen by flow-by, hood, or nasal cannula and sedation with a narcotic and tranquilizer combination.
Epinephrine is given for its bronchodilatory effects in both anaphylaxis (0.01–0.02 mg/kg, IV) and life-threatening asthma (0.02 mg/kg, IM).
Corticosteroids (dexamethasone sodium phosphate, 0.1–0.2 mg/kg, IM or IV) are given for allergic bronchitis, asthma, or severe laryngeal or pharyngeal swelling.
Additionally, bronchodilators, such as aminophylline (3–10 mg/kg, IV or IM), terbutaline (0.01 mg/kg, SC, IM, or slow IV), or albuterol (by nebulization or metered-dose inhaler), can be given if an animal is in crisis.
Diphenhydramine (1–2 mg/kg, IM or IV) is given for allergic reactions.
Also see the calculator on this page for various emergency drug dosages for dogs and cats.
Breathing Disorders in Emergency Treatment of Small Animals
Diagnosis of Breathing Disorders
Changes in respiratory rate or posture
Obviously labored breathing
Changes in mucous membrane color
Respiratory Patterns in Breathing Disorders
Clinical evaluation should first focus on distant and close physical examination before imaging and other diagnostic tests.
Compromised breathing manifests in an increased respiratory rate and effort, immediately followed by a change in the respiratory pattern.
Postural changes follow. Orthopnea is a clinical sign of respiratory distress (see ). Dogs stand with elbows abducted and back arched or high on their rear haunches, with head and neck extended, whereas cats may sit crouched on all four limbs with the sternum slightly elevated.
Obvious labored open-mouth breathing and changes in mucous membrane color (gray, dark pink, or blue [cyanosis]) develop last and indicate substantial loss of pulmonary function and impending pulmonary arrest.

A dog demonstrating orthopnea. Notice the head and neck extension. The elbows are often abducted as well.
Courtesy of Dr. Andrew Linklater.
Location of Pathology in Breathing Disorders
The location of the pathology—pleural space or parenchymal disease—can be determined by careful observation of the breathing pattern and auscultation of the thorax; this will direct therapeutic efforts. Stressful diagnostic procedures, such as radiographs, can lead to rapid decompensation.
Pleural space disease causes asynchronous breathing (also known as an inverse breathing pattern or paradoxical breathing). In normal inspiration, the abdominal wall may expand outward synchronously with the chest wall. In asynchronous breathing, the chest expands on inspiration as the abdomen is pulled inward; then the chest moves inward on expiration as the abdomen expands.
The respiratory pattern is the same, whether air, fluid, or abdominal contents are in the pleural space. Thoracic auscultation reveals muffled lung sounds over the affected regions. Grunting during expiration may be present.
In cats with asynchronous breathing, breathing is slower and more deliberate than in dogs. (See the .)


Flail chest happens when one or more ribs are fractured (usually in multiple places), creating a free segment of the thoracic wall. On inspiration, the normal negative pressure gradient that pulls air into the lungs also pulls on the freely movable segment, making it move inward, opposite of how the rest of the chest moves. (See the .)

Lung parenchymal disease causes quiet or loud breathing, with the chest and abdominal wall moving in the same direction (synchronous breathing). Inspiration and expiration are equally labored, unless concurrent small airway edema or constriction adds an expiratory push.
Thoracic auscultation reveals louder-than-normal lung sounds in early phases. As disease progresses, harsh lung sounds with moist crackles and rales are heard over the affected lungs.
Pulmonary edema, when secondary to cardiac disease, is often accompanied by a murmur, gallop, or arrhythmia and mild hypothermia. Note that a lack of murmur in a cat does not rule out underlying cardiac disease.
The following are differential diagnoses for pulmonary parenchymal disease:
pneumonia (viral, parasitic, fungal, bacterial, aspiration)
acute respiratory distress syndrome or acute lung injury; inflammatory fluid secondary to systemic illness
congestive heart failure (cardiogenic pulmonary edema)
pulmonary contusions or hemorrhage (trauma or coagulopathy)
noncardiogenic pulmonary edema (secondary to seizures, electrocution, or acute airway obstruction [choking or near-drowning]) or reexpansion pulmonary edema
lung lobe torsion
neoplasia
thermal or chemical injury to the lung
Differential diagnoses for respiratory disease (ie, look-alikes) include the following:
central and peripheral neurological disease
severe acidemia (diabetic ketoacidosis, renal failure, toxicosis, or shock)
anemia or altered hemoglobin
nasal occlusion
hyperthermia
opioid administration
cardiac disease
orofacial disease (dental malocclusion or mandibular dislocation or fracture)
other systemic illness (hyperadrenocorticism, hypoglycemia, severe electrolyte changes, hyperthyroidism)
pain, stress, or anxiety
Imaging in Breathing Disorders
Thoracic radiography should be performed only when the animal is able to tolerate the procedure. Radiographs can help differentiate many of these diseases; however, imaging should not delay therapy.
Some animals may be more tolerant of ultrasonography. The TPOCUS can be used to identify pleural fluid or air and clinical signs of "wet lung," examining both hemithoraces at a minimum of 4 points. In this technique, the patient is most often examined in a sternal position, and multiple areas of the chest are examined bilaterally (caudodorsal, several points in the midchest area, as well as cranioventral).
A pneumothorax may be present when the "glide sign" is absent; this is a linear movement noted between the visceral and parietal pleura and requires practice to identify.
B-lines, also called lung rockets, are vertical white projections that arise from the pleural line and occur when there are air-fluid interfaces (see and of B-lines). Small numbers of B-lines may be normal; however, large numbers (ie, more than three) of B-lines can indicate abnormal pulmonary fluid (of any origin).
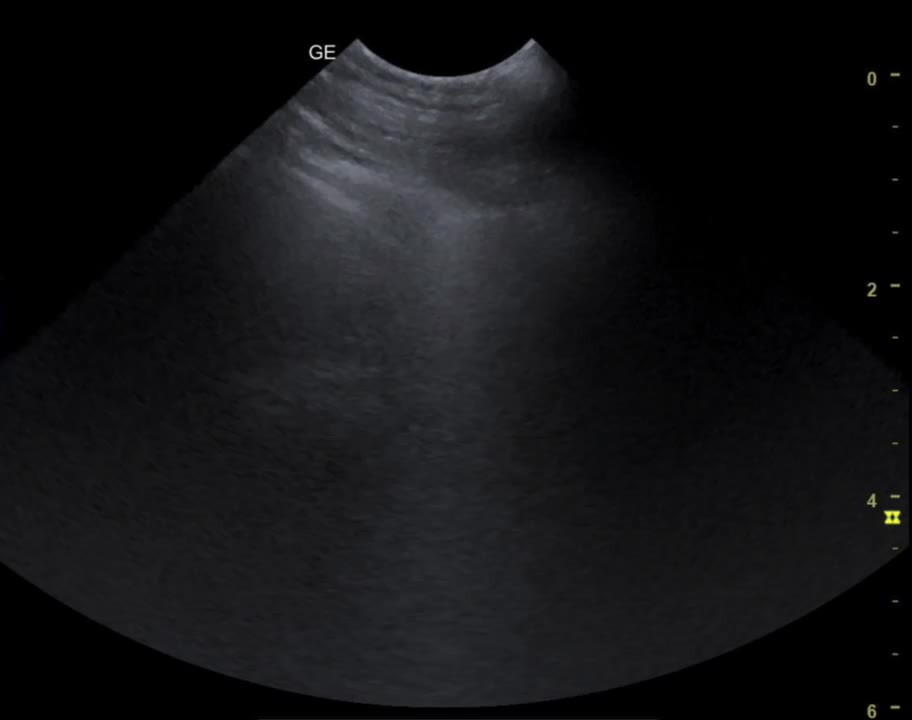


B-lines are bright (hyperechogenic) vertical artifacts that extend from the pleural interface through the screen. They indicate fluid accumulation within the interstitial space.
Courtesy of Dr. Andrew Linklater.
Large amounts of pulmonary fluid often result in irregular lung margins and pleural interface, sometimes called the "shred sign." Large amounts of free pleural fluid are often easy to identify on ultrasonography.
Advanced imaging with CT often provides additional information.
Treatment of Breathing Disorders
Treatment With Oxygen in Breathing Disorders
Oxygen is administered immediately via a variety of methods (see ), including flow-by, mask, hood, nasal, and oxygen cage techniques:
Long-term continuous supplemental oxygen is best provided by a nasal oxygen catheter.
The intranasal oxygen catheter is placed after topical anesthetic has been instilled into the nostril where the tube is to be inserted.
Humidified nasal oxygen flow rates of 50–100 mL/kg/min deliver 40–60% inspired oxygen while allowing the animal to be examined and the underlying disease treated (see ). High-flow nasal oxygen is available at many veterinary specialty centers.
Nasopharyngeal or nasotracheal catheters or bilateral nasal cannulas may provide higher percentages of inspired oxygen.
When patients are placed in oxygen cages, environmental O2 and CO2 levels, humidity, and temperature must be monitored, as substantial alteration of these parameters can be detrimental to patients in an oxygen cage (see ).
Sedation with a narcotic/tranquilizer combination (eg, butorphanol, 0.2–0.4 mg/kg, SC, IM, or IV, with or without acepromazine, 0.01–0.05 mg/kg, SC, IM, or slow IV) can relieve struggling and anxiety.
If cyanosis and decompensation persist or work of breathing is so profound that there is concern over respiratory fatigue, intubation and positive-pressure manual ventilation or mechanical ventilation with 100% oxygen is necessary.


Various methods of oxygen administration to patients: flow-by oxygen (A), cage oxygen (B), nasal oxygen (C), hood oxygen (D), and intubation (E).
Courtesy of Dr. Andrew Linklater.


High-flow nasal oxygen administration to a dog. This method allows a specific percentage of oxygen to be delivered to help avoid invasive mechanical ventilation and oxygen toxicity. Patients tolerate the higher flow rates as the oxygen is warmed and humidified.
Courtesy of Dr. April Blong.


A cat with open-mouth breathing receiving oxygen in an oxygen cage. Note the environmental monitors of oxygen (78.2%), CO2 (1,101 ppm), temperature (22.3°C), and humidity. CO2, measured in parts per million (ppm), should be lowered by ventilating the unit or using a unit with CO2 scavenging or improved cage ventilation when levels are > 2,500 ppm.
Courtesy of Dr. Andrew Linklater.
Treatment for Pleural Space Disease in Breathing Disorders
Catastrophic pleural space disease, with rapid cardiovascular decompensation, absent lung sounds throughout the thorax, and a barrel-shaped thorax, suggests tension pneumothorax. Routine thoracocentesis is often inadequate for affected animals, so an intercostal incision or placement of a large-bore catheter is necessary:
The area over the 5th-9th ribs, in the midthoracic region, is quickly clipped free of hair and prepared in an aseptic fashion.
Lidocaine is injected for local anesthesia.
A small skin incision is made between ribs (at the 7th-8th intercostal space).
Hemostats are used to enter the pleural space, relieving the tension. This allows cardiovascular filling and lung reexpansion.
The open pneumothorax is then managed by placing an indwelling thoracostomy tube and closing the intercostal incision.
Pleural air or fluid without tension pneumothorax should be drained by thoracocentesis.
Before thoracocentesis, sedation with a narcotic-tranquilizer combination (eg, butorphanol, 0.2–0.4 mg/kg, SC, IM, or IV, with or without acepromazine 0.01–0.05 mg/kg, SC, IM, or slow IV) can relieve struggling and anxiety.
For thoracocentesis, a local lidocaine block is often administered, and the following steps are taken:
The intended site is clipped and aseptically prepared.
If fluid is expected, ultrasonographic guidance can be used to identify a fluid pocket. Alternatively, the needle can be inserted ventrally between the sternum and costochondral junction, cranial or caudal to the heart. When air is to be recovered, the needle is inserted into the dorsal half of the thorax, above the costochondral junction.
Usually, an 18- or 20-gauge needle is slowly inserted perpendicular to the thoracic wall, immediately cranial to the rib at the selected location.
An evacuation apparatus (IV extension set, three-way stopcock, and syringe) is attached, and aspiration begins as soon as the pleural space is entered. An alternative is the use of an automatic three-way valve.
The needle is then directed so that it lies within the fluid/air or against the parietal pleura. This prevents lung laceration by the needle as the lung reexpands.
In animals in which the pleural space cannot be emptied (eg, due to tension or continuous pneumothorax, ongoing hemorrhage) or when repeated chest taps are required within minutes to hours, an indwelling thoracostomy tube should be placed for continuous suction.
Investigation of the underlying cause of pleural effusion is always warranted. Often, simple in-house biochemical tests (paired glucose, triglycerides, protein reading) and cytological evaluation will help narrow the differential list.
Hemorrhagic pleural effusion may occur with lung lobe torsion, trauma, or coagulopathies from a variety of underlying diseases.
Chylous pleural effusion can occur with heart disease (cats), neoplasia, lung lobe torsions, or hernias.
Idiopathic chylothorax is a common diagnosis in dogs.
Pyothorax may result secondary to penetrating trauma, migrating foreign bodies, or extension of primary lung disease (pulmonary abscess).
Nonseptic pleural effusion can originate from a multitude of sources, including systemic illness, lung lobe torsion, neoplasia, and more.
Hydrothorax (transudate) may originate from either heart disease, diseases that result in low blood proteins or, less often, venous embolism.
Treatment for Lung Parenchymal Disease in Breathing Disorders
Lung parenchymal disease is primarily treated using oxygen supplementation and sedation to relieve anxiety; specific therapy is directed at the underlying cause.
After initial stabilization, further diagnostic procedures (eg, thoracic imaging and echocardiography) help determine the cause and specific therapy. Sampling of the lungs (direct lung aspirate, tracheal wash, etc) will help determine infectious or inflammatory etiologies but may be contraindicated in patients with severe respiratory compromise. Tracheal wash or bronchoalveolar lavage are often contraindicated in a patient in distress; however, sputum can be examined cytologically as well.
Cardiogenic pulmonary edema is usually associated with a gallop, murmur, arrhythmia, or mild hypothermia.
Cardiogenic pulmonary edema responds well to furosemide administration (2–4 mg/kg, IV or IM in dogs or 0.5–2 mg/kg, IV or IM in cats; 0.25–1 mg/kg/h, IV CRI, in dogs or 0.25–0.6 mg/kg/h, IV CRI, in cats) until respiratory rate or effort improves.
Cardiogenic pulmonary edema may also respond to venodilation from topical nitroglycerin (4–12 mg/kg in dogs, 2–4 mg/kg in cats; ointment quantity [concentration 20 mg/g; 2.5 cm is approximately 15 mg] 1.25-cm strip for larger dogs, 0.3- to 0.6-cm strip for cats) applied to a shaved area of the abdomen, inguinal region, or directly to a mucous membrane; gloves should be worn when handling nitroglycerin ointment.
Severely affected animals with normal blood pressure may benefit from a balanced vasodilator (nitroprusside, 0.5–3 mcg/kg/min, IV [doses up to 10 mcg/kg/min may be required but are aggressive]; or hydralazine, loading dose of 0.1 mg/kg, IV, followed by CRI of 1.5–5 mcg/kg/min, IV). The dosages of these medications are increased slowly while blood pressure is monitored continuously to keep the mean arterial pressure > 85 mm Hg.
Patients with dilated cardiomyopathy may benefit from infusions of dobutamine (2–20 mcg/kg/min, IV CRI, in dogs and 1–5 mcg/kg/min, IV CRI, in cats). Long-term medications such as pimobendan and thromboprophylaxis (eg, clopidogrel or rivaroxaban), ACE inhibitors, angiotensin receptor blockers, or other medications may be indicated as well.
Animals with proteinaceous fluid (as occurs with noncardiogenic pulmonary edema, respiratory distress syndrome, pneumonia, hemorrhage, etc) will not respond to diuretic therapy. Treatment should be directed at the underlying cause (antimicrobials for infectious pneumonia, correction of coagulopathy for hemorrhage, etc).
If oxygen supplementation does not maintain PaO2 > 60 mm Hg (pulse oximetry or SpO2 > 90%), if PaCO2 ≥ 60 mm Hg, if there is moderate to severe increase in work of breathing despite oxygen therapy, or if respiratory failure is imminent, then intubation and manual (with a manual bag valve mask) or mechanical positive-pressure ventilation with 100% oxygen is required while the underlying disease is treated. Suction should be available to help clear the airway.
Physical maneuvers may help to clear the lungs or airway of fulminant disease; elevated or postural pulmonary parenchymal evacuation (EPPE) can be performed with two or more people elevating the pet vertically, head down, while guarding the endotracheal tube (see ). The thoracic cavity should be manually compressed to assist airway and lung fluid drainage. Manual ventilation with 100% oxygen and suction of the airway should be performed between EPPE efforts.
Occasionally, surgical procedures may be necessary to alleviate severe hypoxemia to improve ventilation/perfusion (V/Q) mismatches (eg, lobectomy for consolidation or lung lobe torsion or repair of a diaphragmatic hernia).


Dachshund with a ruptured chordae and in fulminant congestive heart failure undergoing elevated pulmonary parenchymal evaluation (EPPE) to help drain large amounts of fluid from the respiratory tract. The patient was intubated and then inverted between periods of positive pressure ventilation, while steady pressure was applied to the chest to evacuate fluid.
Courtesy of Dr. Andrew Linklater.
Circulatory Disorders in Small Animal Emergency Patients
Diagnosis of Circulatory Disorders
Animals with circulatory compromise can have alterations in the following physical perfusion parameters (see also the table ):
heart rate
mucous membrane color
CRT
rectal temperature
pulse quality
level of consciousness
Careful auscultation of the heart (for a murmur, gallop, or arrhythmia, or for muffled heart sounds) and lungs (for evidence of fluid) is important to help identify heart failure as a cause of poor perfusion.
Measurements of direct or indirect arterial blood pressure, central venous pressure, central venous PaO2, and serum lactate concentration provide objective data for reaching resuscitation end points and monitoring trends of change after resuscitation.
A thorough history and physical examination will help identify the reason for shock.
Shock generally progresses through three stages:
In the early compensatory stage of hypovolemic shock, clinical signs in dogs include tachycardia, pink to red mucous membranes, rapid CRT, and bounding pulses; the patient is most often alert and responsive. Dogs with substantial pain or anxiety may appear to be in compensatory shock, so administration of appropriate analgesics is warranted, along with allowing time for the patient to acclimate to the environment. Tachycardia is often the first and only clinical sign, so persistent tachycardia must be considered a sign of altered perfusion. This stage is rarely identified in cats.
In the middle stage of shock (also called the early decompensatory stage), dogs begin to have pale mucous membranes, prolonged CRT, weak pulses, tachycardia, and a decreased level of responsiveness. Cats have gray mucous membranes, slow CRT, weak or absent pulses, hypothermia, and a normal or low heart rate.
As shock approaches the terminal (or late decompensatory) stage, the heart rate slows in both dogs and cats, and animals begin to lose consciousness. Clinical signs in this terminal stage include bradycardia, severe hypotension, absent pulses, gray or ashen mucous membranes, prolonged CRT, depressed or altered mentation, oliguria, and abnormal respiratory patterns. Cardiopulmonary arrest is a common sequela.
Treatment of Circulatory Disorders
The therapeutic goal with shock is to deliver oxygen and glucose to the tissues. This requires not only effective cardiac blood pumping but also adequate hemoglobin, intravascular volume, and vascular tone and patency, along with sufficient oxygen and glucose for cellular metabolism.
General guidelines for treatment of hypovolemic and distributive shock are described below; however, modifications may be needed for specific animals or disease processes. (See also Fluid Therapy in Animals.)
Oxygen Supplementation in Circulatory Disorders
Oxygen (at least 40–60% inspired concentration) should be administered to unstable patients until it is determined that they no longer require oxygen based on respiratory rate, effort, pulse oximetry (or arterial blood gas evaluation), and resolution of the underlying disease. Various techniques of oxygen administration are listed in increasing percentage of oxygen delivered, depending on the rate administered (see also ):
flow-by technique (25–40%)
hood (30–40%)
mask (35–60%)
cage (50–70%)
nasal cannula (50–70%)
nasotracheal or transtracheal catheter (up to 80%)
high-flow nasal cannula (adjusted 21–100%)
endotracheal tube (up to 100%)
Hyperbaric oxygen is usually inappropriate during the initial assessment because access to the patient is limited.
Each of these techniques has advantages and disadvantages, depending on the patient's injuries, tolerability of the technique, and patient access. Monitoring the patient's vital signs, including respiratory rate and effort, is essential; SpO2 measurement is tolerated in some conscious patients; however, blood gas analysis is usually reserved for those who are anesthetized or comatose.
If patients are not achieving improved oxygenation (PaO2 remains < 70 mm Hg) or ventilation (PaCO2 remains > 50 mm Hg) with these techniques, mechanical ventilation is usually indicated.Over time, oxygen can become toxic to the respiratory epithelium; the goal should be to decrease inspired oxygen concentration to < 50% within 24 hours.
Pearls & Pitfalls
|
Intravascular Volume Replacement in Circulatory Disorders
IV catheters are used for intravascular volume replacement, with multiple catheters placed for rapid, large-volume infusion in larger patients. Intraosseous catheters may be used as an alternative.
Isotonic crystalloids can be administered by low-volume (10–15 mL/kg, IV) or high-volume (20–30 mL/kg, IV) boluses, each delivered over 10–15 minutes until desired end points of resuscitation are reached.
The concurrent use of colloids (blood products or hydroxyethyl starch, 2–10 mL/kg, IV bolus) can decrease the amount of crystalloid required, rapidly expand the intravascular space with a smaller volume of fluid infused, and decrease the amount of fluid extravasating into the interstitial spaces of vital organs (eg, lung, brain). For an in-depth explanation, see Fluid Therapy in Animals
Hypertonic saline solution (HTS) (7%) at a dosage of 4 mL/kg, IV, should not be used in patients that are dehydrated or that are at risk for hypernatremia; HTS may be beneficial in patients with traumatic brain injury and may also improve cardiac contractility.
Concerns about the use of hydroxyethyl starch solutions resulting in acute kidney injury in veterinary patients have not been described when 6% solutions (mean molecular weight, 130 kDa; degree of substitution, 0.4) are used for < 24 hours; coagulation is also not impacted until > 50 mL/kg are administered (9, 10, 11, 12).
Small-volume resuscitation with low-normal end points (normal perfusion parameters with a mean arterial pressure of 60–80 mm Hg) is used to avoid volume overload and hypertension (which may exacerbate hemorrhage). This technique is ideal for animals with head injury, pulmonary edema or contusions, hemorrhage, or heart disease, and for all cats in hypovolemic shock, as they have a smaller blood volume.
Large-volume resuscitation with high-normal end points (normal perfusion parameters with a mean arterial pressure of 80–100 mm Hg) is used in patients with GI disease, sepsis, or systemic vasodilation. The smallest amount of crystalloids and colloids possible is used to obtain and maintain a systolic blood pressure of 90 mm Hg, restore a normal heart rate, and improve CRT and pulses. For patients not responding to intravascular volume resuscitation, pressor medications should be added next. For an in-depth explanation, see Fluid Therapy in Animals.
Corticosteroids in Circulatory Disorders
Corticosteroids are administered when a deficiency is suspected (ie, hypoadrenocorticism, critical illness–related corticosteroid insufficiency [CIRCI]). High-dose steroid administration has not been proven to lower mortality rates in hypovolemic, septic, or cardiogenic shock and has been associated with increased morbidity, so it is not recommended.
Cardiovascular Support in Circulatory Disorders
Pharmacological agents (positive inotropes, systemic vasopressors) can be used when fluid infusion has adequately replaced intravascular volume but fails to restore blood pressure and perfusion, or when poor cardiac contractility is thought to contribute to hypotension.
A positive inotropic agent can be administered to increase cardiac contractility in diseases such as sepsis and dilated cardiomyopathy (eg, dobutamine, 2–20 mcg/kg/min, IV CRI, initial dose 2–5 mcg/kg/min, and the dosage titrated for optimal cardiac output).
Pressor agents delivered as an IV CRI, such as dopamine (5–20 mcg/kg/min), norepinephrine (0.05–2 mcg/kg/min), epinephrine (0.125–2 mcg/kg/min), phenylephrine (1–3 mcg/kg/min), and vasopressin (0.5–5 mU/kg/min), are other options to support blood pressure. These drugs should be delivered in the smallest dosage needed to maintain arterial systolic pressure of > 90 mm Hg.
Hemoglobin-based oxygen-carrying fluids have been used for patients with concurrent anemia and hypotension; however, they are not currently available in may countries.
The blood flow to the kidneys and GI tract, as well as to other organs, may have been seriously impaired during shock. Urine output, heart rate, blood pressure, ECG, pulse intensity, and mucous membrane color should be closely monitored because further vasoconstriction can worsen organ blood flow and function.
If organ function declines or if arrhythmias become a problem, administration of the vasopressor should be stopped.
Disability Disorders in Small Animal Emergency Patients
Diagnosis and Treatment of Disability Disorders
Acute presentation of trauma or other neurological disorders often warrants immediate and timely assessment and intervention. A thorough physical examination should occur to localize the severity and location of disease, which can be accomplished on a physical and neurological examination. A differential list should be developed for any patient with a neurological problem, using the DAMNITV scheme (degenerative; anomalous; metabolic; neoplastic or nutritional; inflammatory, infectious, and idiopathic; traumatic or toxic; and vascular etiologies). Examples of disability that occur in emergency patients can include the following:
head trauma (see )
spinal trauma
acute inability to walk or ambulate normally
seizures
altered mentation (level of consciousness)
See also additional resources on performing a neurological examination with localization of the disease.
Traumatic brain injury (TBI) is divided into primary and secondary injury; the primary injury is what occurs at the initial time of injury (laceration, hemorrhage, etc), whereas secondary injury occurs after the primary is complete, resulting from the metabolic derangements that can occur afterwards, such as swelling and inflammation. Secondary injury is exacerbated by changes at the cellular level, including accumulation of intracellular calcium, release of the excitatory neurotransmitter glutamate, etc. Patients should be monitored closely using the modified Glasgow Coma Scale (MGCS).

This puppy was bitten by another dog in the household. Note the injury on the left side of the dog's cranium; there is an open wound and cranial depression.
Courtesy of Dr. Andrew Linklater.
Treatment of TBI and other serious intracranial disease has two facets.
The first principle in treatment of TBI is to cause no further harm by treating or avoiding metabolic problems that can exacerbate intracranial disease, including the following:
Correcting hypotension to optimize blood flow to the brain. This involves addressing other parameters discussed in this chapter (fluid administration, pressors, arresting hemorrhage, etc).
Correcting hypoxemia to optimize oxygen delivery to the brain. This involves titrating oxygen therapy to optimize oxygen delivery to tissues with oxygen supplementation or mechanical ventilation.
Correcting hyper- or hypocapnia (hyper- or hypoventilation) to optimize cerebral blood flow. This requires mechanical ventilation for patients whose partial pressure of carbon dioxide exceeds 45 mm Hg (venous) or 40 mm Hg (arterial). Hyperventilation should be avoided.
Avoiding hyper- and hypoglycemia and severe electrolyte and acid-base disturbances to optimize cerebral metabolism.
Avoiding hyperthermia to avoid cerebral injury. Hyperthermia can exacerbate the metabolic derangements in TBI, and although routinely recommended in human medicine to target therapeutic hypothermia of 32–34°C, therapeutic hypothermia is rarely used in veterinary patients. The use of therapeutic hypothermia can have many complications, impacting many body systems and resulting in shivering, so anesthesia and mechanical ventilation are often required.
Often, short-acting medications (such as fentanyl) or multimodal analgesia is necessary, especially to avoid some of the complications that may occur as a side effect of large doses of opioids. (See Pain Control.)
Careful manipulation involves avoiding obstruction of the cerebral venous drainage by avoiding manipulation of the neck and occlusion of the jugular veins for repeated phlebotomy or central line placement. Placement of nasal oxygen lines and feeding tubes may result in sneezing, which can increase intracranial pressure.
The second aspect of treating TBI is specific therapy for intracranial disease. Patients should receive hyperosmolar therapy, with the cautious administration of either mannitol (0.25–1 g/kg, IV through a filter) or hypertonic saline solution (2–4 mL/kg, IV), particularly those patients with a deteriorating mental status or MGCS score. Attempting to decrease cerebral volume with elevation of the patient's head by 15–30° (while keeping the neck in a neutral position) may decrease cerebral blood volume without impacting cerebral perfusion pressure. Anticonvulsant drugs are not routinely recommended prophylactically in veterinary patients but are indicated if seizures occur; seizures increase the metabolic demand and glutamate concentration in the brain, exacerbating intracranial disease.
Very limited information has been published on veterinary TBI patients; levetiracetam is routinely recommended because of its wide safety margins and ability to monitor MGCS. Steroids and furosemide have no proven benefit in these patients.
Acute spinal injury most commonly will occur either from trauma or intervertebral disk disease. A patient that has suffered spinal trauma should be approached in a similar manner to a patient with TBI. Additionally, the patient should be immediately immobilized (restrained on a back board) until evaluation and imaging are complete. Localizing the disease based on reflexes and paresis is important for more information on severity and for prognostication.
Seizures are a common presentation to the emergency room. Careful attention to the owner-provided history and a thorough physical examination are essential to help differentiate a seizure from a syncopal episode or other systemic or neurological conditions. Causes are generally divided into intracranial and extracranial, and epilepsy is a diagnosis of rule out. Routine bloodwork (CBC, chemistry, electrolyte) panels, urinalysis, and infectious disease testing (eg, feline leukemia virus, feline immunodeficiency virus, tickborne or fungal diseases) are recommended before systemic imaging (eg, thoracic radiography, abdominal sonography) and MRI and CSF analysis.
Presuming no identified causes, emergency management of seizures is often recommended with one of the following medications: benzodiazepine (diazepam, 0.5 mg/kg, IV or 1–2 mg/kg, per rectum, or midazolam, 0.1–0.25 mg/kg, IV or 0.2 mg/kg, intranasally; these may also be given as a CRI if seizures are prolonged or repeated: diazepam, 0.2–2 mg/kg/h through a dedicated catheter and protected from light, or midazolam, 0.25–0.4 mg/kg/h, CRI); phenobarbital (4–6 mg/kg, IV, every 6 hours up to 20 mg/kg total, monitoring the patient's mental status closely; this often results in prolonged sedation); levetiracetam (20–60 mg/kg, every 8 hours); propofol (1–4 mg/kg, slowly for induction, then 0.1–0.6 mg/kg/min CRI; these patients often require intubation and mechanical ventilation) (13, 14).
Other medications used with varying success include ketamine, dexmedetomidine, and acepromazine. Addressing intracranial pressure as discussed above, if present, is essential.
The neurological system can present with a variety of other clinical signs. It is important to perform a complete physical and neurological examination to identify the location and severity of disease. Altered mentation can occur from simple problems such as hypoglycemia, which is easily identified with a bedside glucometer and treated with IV dextrose; however, the causes of hypoglycemia are quite wide (eg, poor nutrition, especially in young or emaciated animals; insulin overdose; liver failure). Hyperammonemia can be treated with lactulose. Patients should have a thorough systemic workup to rule out extracranial causes of altered mentation. If extracranial causes of altered mentation have been ruled out, many patients may need advanced imaging to check for intracranial disease, such as meningitis, and tumors.
Exposure Risk in Small Animal Emergency Patients
Diagnosis of Exposure and Environmental Disorders
Acute presentation of emergency patients, especially with trauma, puts them at risk for hypothermia, particularly from exposed wounds. This aspect of assessment is meant to ensure that the entire animal is examined for any open wounds, wounds are addressed appropriately, and risk factors for hypothermia are identified.
It take several weeks for even minor wounds to completely heal and to ensure that no complications develop. However, extensive wounds require not only appropriate early management but likely substantial and ongoing open wound care and/or delayed surgical procedures to fully address injuries. Often, the extent of the wounds cannot be identified at the time of initial injury, because blood supply disruption may not be clinically evident.
Treatment of Exposure and Environmental Disorders
Several principles govern the treatment of emergency patients with wounds. Addressing the other XABCDE parameters is vital to ensuring the patient survives in the short term; Analgesia is essential for these patients as well. For wound care in emergency patients, the following initial steps should be performed:
A sterile water-soluble lubricant can be applied to an open wound to help prevent desiccation and may help prevent accumulation of debris (hair) as the surrounding area is clipped and cleaned. Keeping the wound moist may also help optimize wound healing.
Prevention of further injury and contamination often requires application of a sterile dressing (bandage) as soon as possible and handling any open wounds in an aseptic manner (washed, gloved hands; sterile instruments). Bandage placement also helps immobilize the area; an Elizabethan collar should be used to prevent self-trauma.
Wound hemostasis also helps prevent accumulation of blood (hematomas) in tissues, which can complicate or delay healing.
As the patient is stabilized, definitive wound management may be possible and often requires heavy sedation or general anesthesia.
Several steps are used to optimize the stages of wound healing. With large, contaminated wounds, often there is substantial contamination, requiring open wound management to allow tissue to declare as necrotic or viable and to help minimize contamination. Open wound management is required in several situations:
if it is not known whether the tissue is necrotic
if the wound is obviously infected (purulent discharge, foul odor, intracellular bacteria on cytological evaluation, or positive bacterial growth on culture
if the wound is > 12 hours old
if excessive tension would be placed on sutures
Many small, uncontaminated wounds may be closed primarily; however, the extent of the wound should be determined by probing because the most superficial part of the wound may not represent the full extent of the wound (see ; see also ).

Bite wounds may initially appear minor, but they are connected underneath the skin with extensive underlying tissue damage.
Courtesy of Dr. Andrew Linklater.

Dog with substantial degloving wounds after being rolled over by a car. The chest is to the right, and the right hind leg has been lifted to expose the large wounds on the ventral abdomen.
Courtesy of Dr. Andrew Linklater.
The steps of initial wound management include the following:
Obviously necrotic tissue should be sharply debrided back to healthy, bleeding tissue. Embedded debris should also be also removed.
With large, contaminated wounds, irrigation with tap water may be appropriate to start but is not ideal. For smaller wounds or as a final step for large wounds, irrigation techniques using sterile solutions (such as sterile 0.9% saline solution or lactated Ringer's solution) are often recommended. There is controversy regarding both the addition of antiseptic agents to lavage fluids and the ideal pressure to lavage wounds without causing further harm. A pressure of 8–12 psi is ideal but may be exceeded with the commonly recommended 35-cc syringe and 22-gauge needle or catheter. A volume of 50-–100 mL of irrigation fluid per cm2 of wound has been recommended. Cultures should be obtained after irrigation to help direct antimicrobial therapy.
Appropriate wound care is likely superior to application of any topical antiseptic agents; however, in a highly infected wound, medical-grade manuka honey has several properties that often improve healing. Wet-to-dry bandages were traditionally recommended to assist with debridement; however, controversy exists regarding their use.
Elimination of dead space with bandages, sutures, or drains will help prevent fluid accumulation; drain sites should be covered to help minimize contamination and are usually removed in several days when fluid accumulation is 0.2 mL/kg/h or less.
Wounds may be sutured closed (primary intention healing) if the wound is fresh, the tissue appears healthy, and no infection is present. Otherwise, delayed primary closure (3–5 days later)—ensuring viable tissue and no infection after wound management—or second intention (open wound management) may occur, with regular bandage changes performed every 12–72 hours. More information on wound management and healing is provided in For More Information.
Warming the Hypothermic Patient
Another important aspect of exposure is patient hypothermia. Hypothermia in emergency patients can be detrimental in several ways, including shock (especially in cats), impaired drug metabolism, impaired wound healing, and abnormal coagulation. It is also not uncommon for patients to become hypothermic in the veterinary hospital due to low ambient temperature, open wounds, anesthesia, and administration of room-temperature fluids.
Small, young, and old animals are at higher risk of hypothermia. Animals in shock should be slowly warmed during fluid resuscitation until rectal temperatures are > 36.5°C (98°F). This is best accomplished by increasing the environmental temperature using warm air blowers, warm water blankets, and IV fluid warmers; however, the effectiveness of some of these techniques has not been clearly demonstrated. Hot water bottles and hot rice bags should be avoided because of potential burn risk.
Gastric, peritoneal, or urinary lavage may be needed for severe hypothermia.
Surface warming is instituted only after initial volume resuscitation has provided enough intravascular volume to offset peripheral vasodilation. Care must be taken in animals with cardiogenic shock or pericardial disease to avoid excessive peripheral vasodilation, because this may exacerbate a relative hypovolemia (due to decreased cardiac output).
In patients requiring surgery or anesthesia, reflective blankets and wool foot covers can help minimize drops in body temperature.
Pain Control
Analgesia is provided as indicated during initial fluid resuscitation for optimal cardiovascular response and relief of anxiety and pain.
Ideally, pure mu opioid receptor agonists are often the first-line agents because they are potent, have minimal cardiovascular effects, and are reversible. Common agents include methadone (0.1–0.5 mg/kg, IV), hydromorphone (0.1–0.2 mg/kg, IV), fentanyl (5–10 mcg/kg loading dose followed by 3–10 mcg/kg/h, IV CRI); butorphanol is less effective with severe pain. Multimodal analgesia, with addition of lidocaine, and/or ketamine infusions may be essential in some patients. Neuroleptanalgesia may be necessary in some patients with the addition of sedatives such as acepromazine (if there is no risk of hypotension), benzodiazepines, or trazodone.
Local anesthetic techniques can be applied in a variety of conditions, including the need for surgery with liposome-encapsulated bupivicaine for planned surgical procedures. Additional oral or injectable medications (eg, nonsteroidal anti-inflammatory agents, gabapentin, tramadol, amantidine) may be added, depending on the patient's GI and renal functions and ability to tolerate oral medications. Adjuvant therapy for analgesia, such as laser therapy, acupuncture, or other energy-emitting techniques (extracorporeal shock wave therapy or pulsed electromagnetic therapy), may also benefit some patients.
Multimodal analgesia using a combination of medications, routes, techniques, and methods of administration is often essential. (See also Pain Assessment and Management.)
Key Points
A primary survey is essential to identify patients that require rapid intervention to avoid rapid deterioration.
XABCDE (eXsanguination, airway, breathing, circulation, disability [neurological problems including level of consciousness], exposure risk) should all be rapidly evaluated.
Identification of the cause of shock, along with rapid arrest of hemorrhage and administration of IV fluids and vasopressor agents, is essential.
Pain control is an essential part of emergency care.
Monitoring patients for response to therapy and need for additional intervention is key.
For More Information
Drobatz KJ, Hopper K, Roanski EA, Silverstein DC, eds. Textbook of Small Animal Emergency Medicine. Wiley-Blackwell; 2018.
Kirby R, Linklater A, eds. Monitoring and Intervention for the Critically Ill Small Animal: The Rule of 20. Wiley-Blackwell; 2017.
Also see pet owner content regarding emergency care for dogs and cats.
References
LeVine DN, Goggs R, Kohn B, et al. ACVIM consensus statement on the treatment of immune thrombocytopenia in dogs and cats. J Vet Intern Med. 2024;38(4):1982-2007. doi:10.1111/jvim.17079
Li, R. Acquired coagulopathy. In: Drobatz KJ, Hopper K, Roanski EA, Silverstein DC, eds. Textbook of Small Animal Emergency Medicine. Wiley-Blackwell; 2018:444-454. doi:10.1002/9781119028994.ch70
Kirby R, Linklater A, eds. Monitoring and Intervention for the Critically Ill Small Animal: The Rule of 20. Wiley-Blackwell; 2017. doi:10.1002/9781118923870
Brown JC, Brainard BM, Fletcher DJ, Nie B, Arnold RD, Schmiedt CW. Effect of aminocaproic acid on clot strength and clot lysis of canine blood determined by use of an in vitro model of hyperfibrinolysis. Am J Vet Res. 2016;77(11):1258-1265. doi:10.2460/ajvr.77.11.1258
Kelmer E, Segev G, Papashvilli V, et al. Effects of intravenous administration of tranexamic acid on hematological, hemostatic, and thromboelastographic analytes in healthy adult dogs. J Vet Emerg Crit Care (San Antonio). 2015;25(4):495-501. doi:10.1111/vec.12319
Sigrist NE, Hofer-Inteeworn N, Schefer RJ, Kuemmerle-Fraune C, Schnyder M, Kutter APN. Hyperfibrinolysis and hypofibrinogenemia diagnosed with rotational thromboelastometry in dogs naturally infected with Angiostrongylus vasorum. J Vet Intern Med. 2017;31(4):1091-1099. doi:10.1111/jvim.14723
Kraus KH, Turrentine MA, Jergens AE, Johnson GS. Effect of desmopressin acetate on bleeding times and plasma von Willebrand factor in Doberman Pinscher dogs with von Willebrand’s disease. Vet Surg. 1989;18(2):103-109. doi:10.1111/j.1532-950X.1989.tb01051.x
Whitley NT, Corzo‐Menendez N, Carmichael NG, McGarry JW. Cerebral and conjunctival haemorrhages associated with von Willebrand factor deficiency and canine angiostrongylosis. J Small Anim Pract. 2005;46(2):75-78. doi:10.1111/j.1748-5827.2005.tb00296.x
Sigrist NE, Kälin N, Dreyfus A. Effects of hydroxyethyl starch 130/0.4 on serum creatinine concentration and development of acute kidney injury in nonazotemic cats. J Vet Intern Med. 2017;31(6):1749-1756. doi:10.1111/jvim.148131
Sigrist NE, Kälin N, Dreyfus A. Changes in serum creatinine concentration and acute kidney injury (AKI) grade in dogs treated with hydroxyethyl starch 130/0.4 from 2013 to 2015. J Vet Intern Med. 2017;31(2):434-441. doi:10.1111/jvim.14645
Boyd CJ, Sharp CR, Claus MA, Raisis AL, Hosgood G, Smart L. Prospective randomized controlled blinded clinical trial evaluating biomarkers of acute kidney injury following 6% hydroxyethyl starch 130/0.4 or Hartmann's solution in dogs. J Vet Emerg Crit Care (San Antonio). 2021;31(3):306-314. doi:10.1111/vec.130563
Diniz MS, Teixeira-Neto FJ, Celeita-Rodríguez N, et al. Effects of 6% tetrastarch and lactated Ringer's solution on extravascular lung water and markers of acute renal injury in hemorrhaged, isoflurane-anesthetized healthy dogs. J Vet Intern Med. 2018;32(2):712-721. doi:10.1111/jvim.148534.
Charamlambous M, Bhatti SFM, Van Ham L, et al. Intranasal midazolam versus rectal diazepam for the management of canine status epilepticus: a multicenter randomized parallel-group clinical trial. J Vet Intern Med. 2017;31(4):1149-1115. doi:org/10.1111/jvim.14734
Benedicenti L, Galban EM. Seizures. In: Drobatz KJ, Hopper H, Rozanski E, Silverstein DC, eds. Textbook of Small Animal Emergency Medicine. Wiley-Blackwell; 2019:124-130. doi:10.1002/9781119028994.ch21





