

Duck viral hepatitis is an acute infectious disease affecting young ducklings. It is associated with high mortality and characteristic liver lesions. Diagnosis is by viral isolation or PCR assay. Vaccination and biosecurity controls can be used for prevention. There is no specific treatment for infected ducks.
Duck viral hepatitis (DVH) is an acute, highly infectious viral disease typically affecting ducklings less than six weeks old. DVH is characterized by a short incubation period, sudden onset, high mortality, and characteristic liver lesions.
The viruses that cause DVH in ducklings should not be confused with duck hepatitis B virus, a hepadnavirus infection of older ducks.
Etiology of Duck Viral Hepatitis
Duck viral hepatitis (DVH) was historically subdivided into types I, II, and III. The originally described DVH type I is caused by one of at least three genotypes of duck hepatitis A virus (DHAV) of the genus Avihepatovirus in the Picornaviridae family. The most widespread and virulent is DHAV type 1 (DHAV-1).
Two antigenically distinct genotypes have been identified in Taiwan (DHAV-2) and in China and the Republic of Korea (DHAV-3).
DHAV is readily propagated in chicken and duck embryos, and they do not produce hemagglutinins. Field experience with DHAV-1 indicates that egg transmission does not occur. The disease can be transmitted experimentally by parenteral or oral administration of infected tissues.
Viruses that differ from DHAV have been recognized as additional causes of DVH in ducklings. DVH type II, now classified as duck astrovirus type 1 (DAstV-1), is difficult to propagate under laboratory conditions. DVH type III is also now classified as an astrovirus (DAstV-2) and can be propagated in duck (but not chicken) embryos.
At least 10 genera of hepatotropic viruses across at least 6 viral families have been implicated in DVH disease, which further complicates disease classification.
Clinical Findings of Duck Viral Hepatitis
The incubation period for duck hepatitis A virus is 18–48 hours. Affected ducklings become lethargic, lose balance, paddle spasmodically, and die within minutes, typically with opisthotonos.
Although adults may become infected, clinical signs of disease have not been seen in ducks > 7 weeks old. Mortality may be up to 95% in fully susceptible ducklings. Practically all deaths occur ≤ 1 week after onset of clinical signs.
Pearls & Pitfalls
|
The clinical course of DAstV-1 infection is similar to that of DHAV-1 and can be seen in ducklings immune to DHAV-1 infection.
DAstV-2 infections are seen in ducklings despite immunity to DHAV-1. The clinical course of DAstV-2 infection is less severe, and mortality is rarely > 30%.
Lesions

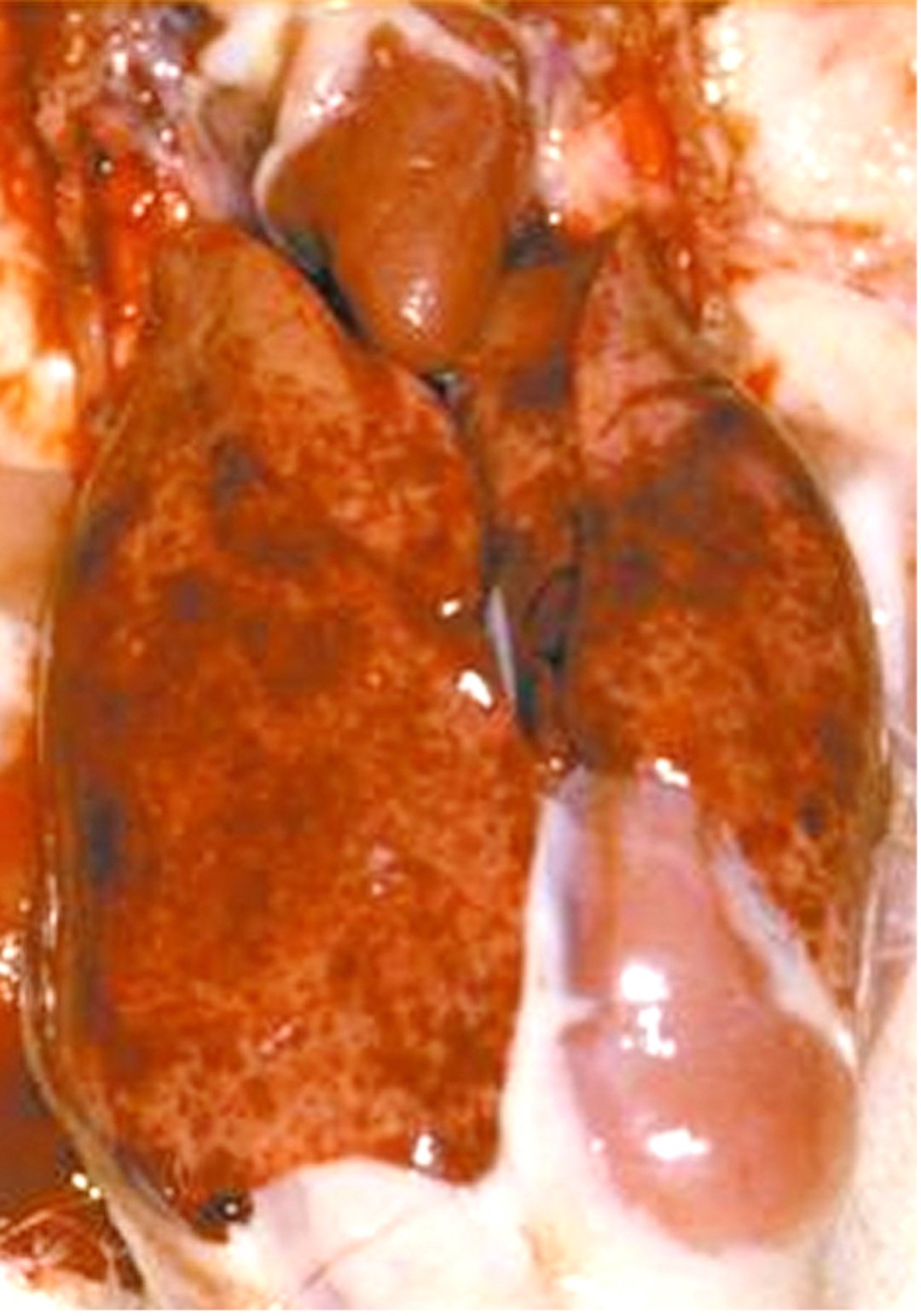
Duck hepatitis A virus type 1 infection in a commercial Pekin duckling. Note extensive petechial and ecchymotic hemorrhages throughout the liver.
Courtesy of Dr. Peter R. Woolcock.
The lesions caused by the viral genotypes inducing DVH are similar:
The liver is enlarged and covered with hemorrhagic foci.
The spleen may be enlarged and mottled.
Kidneys may be enlarged and renal blood vessels congested.
Diagnosis of Duck Viral Hepatitis
History and lesions
Confirmation via virus isolation or PCR assay
A presumptive diagnosis of duck viral hepatitis can be based on the history and lesions. Sudden onset, rapid transmission, and a short clinical course, together with characteristic liver lesions, are highly suggestive of duck viral hepatitis.
Confirmatory diagnosis of DVH requires detection of the viral etiologic agent, usually from liver homogenate. Immunologic antibody detection tests have little value in the diagnosis of acute infection.
DHAV-1 may be isolated in duck embryos and duck-embryo liver cell cultures, or less easily in chicken embryos. The virus can also be identified by virus neutralization with specific antisera or by inoculation into both susceptible and immune day-old ducklings. DAstV-1 and DAstV-2 are not neutralized by classic DHAV-1 antiserum.
DHAV, DAstV-1, and DAstV-2 can be identified by RT-PCR assay. Several multiplex RT-PCR tests have been developed for differentiation of the DHAV genotypes.
Prevention and Treatment of Duck Viral Hepatitis
No specific treatment
Vaccination and biosecurity
There is no specific treatment for duck viral hepatitis infection. Prevention and control are based on strict biosecurity and implementation of vaccination protocols.
Strict isolation, particularly during the first 5 weeks of life, is recommended. Contact with wild waterfowl should be avoided. Rats have been reported as a reservoir host of the virus; therefore, pest control is indicated.
Immunization of breeder ducks with modified live virus vaccines, using DHAV, DAstV-1, and DAstV-2, provides parenteral immunity that effectively prevents high losses in young ducklings. The DHAV-1 vaccine is administered SC in the neck to breeder ducks at 16, 20, and 24 weeks and every 12 weeks thereafter throughout the laying period. Three immunizations are advisable for passive protection of ducklings.
An inactivated DHAV-1 vaccine for use in breeder ducks that have been previously primed with live DHAV-1 has been described. A single dose of the inactivated vaccine, administered IM before the birds come into lay, provides passive immunity for a complete laying cycle to progeny ducklings.
The chick-embryo origin, modified live DHAV-1 vaccine also can be used for early vaccination of ducklings susceptible to DHAV-1 (progeny of nonimmune breeders). This vaccine is administered SC or by foot web stab in a single dose to day-old ducklings. Vaccinated ducklings rapidly develop an active immunity within 3–4 days.
Antibody against DHAV-1, prepared from the eggs of hyperimmunized chickens and administered SC in the neck at the time of initial loss, is an effective flock treatment.
Key Points
The clinical and pathologic presentation of duck viral hepatitis in susceptible ducklings is attributed to several viral etiologic agents across multiple families.
Duck viral hepatitis pathology can be induced by at least three genotypes of duck hepatitis A virus as well as DAstV-1 and DAstV-2.
Antigen detection is typically the focus of diagnosis, whereas serologic tests can be used for serologic and epidemiologic surveillance.
Management is based on biosecurity as well as implementation of appropriate vaccination protocols.
For More Information
Duck virus hepatitis. Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (Terrestrial Manual) of the World Organisation for Animal Health. 2018.


