



Laryngeal hemiplegia is a progressive neuropathy of the recurrent laryngeal nerve, leading to atrophy and dysfunction of the cricoarytenoideus dorsalis muscle, an important abductor for the arytenoid cartilage. This leads to an inability to abduct the arytenoid cartilage and vocal fold away from the airway during inspiration (manifested as an inspiratory noise referred to as a “roar”), causing a reduction in airflow (causing poor performance and/or exercise intolerance). Endoscopy (static and/or dynamic) is necessary for diagnosis. Treatment is dependent on the presenting complaint, intended use, and extent of arytenoid dysfunction and includes laryngeal reinnervation, ventriculectomy, ventriculocordectomy, prosthetic laryngoplasty (“tie-back”), or partial arytenoidectomy.
Etiology and Pathogenesis of Laryngeal Hemiplegia in Horses

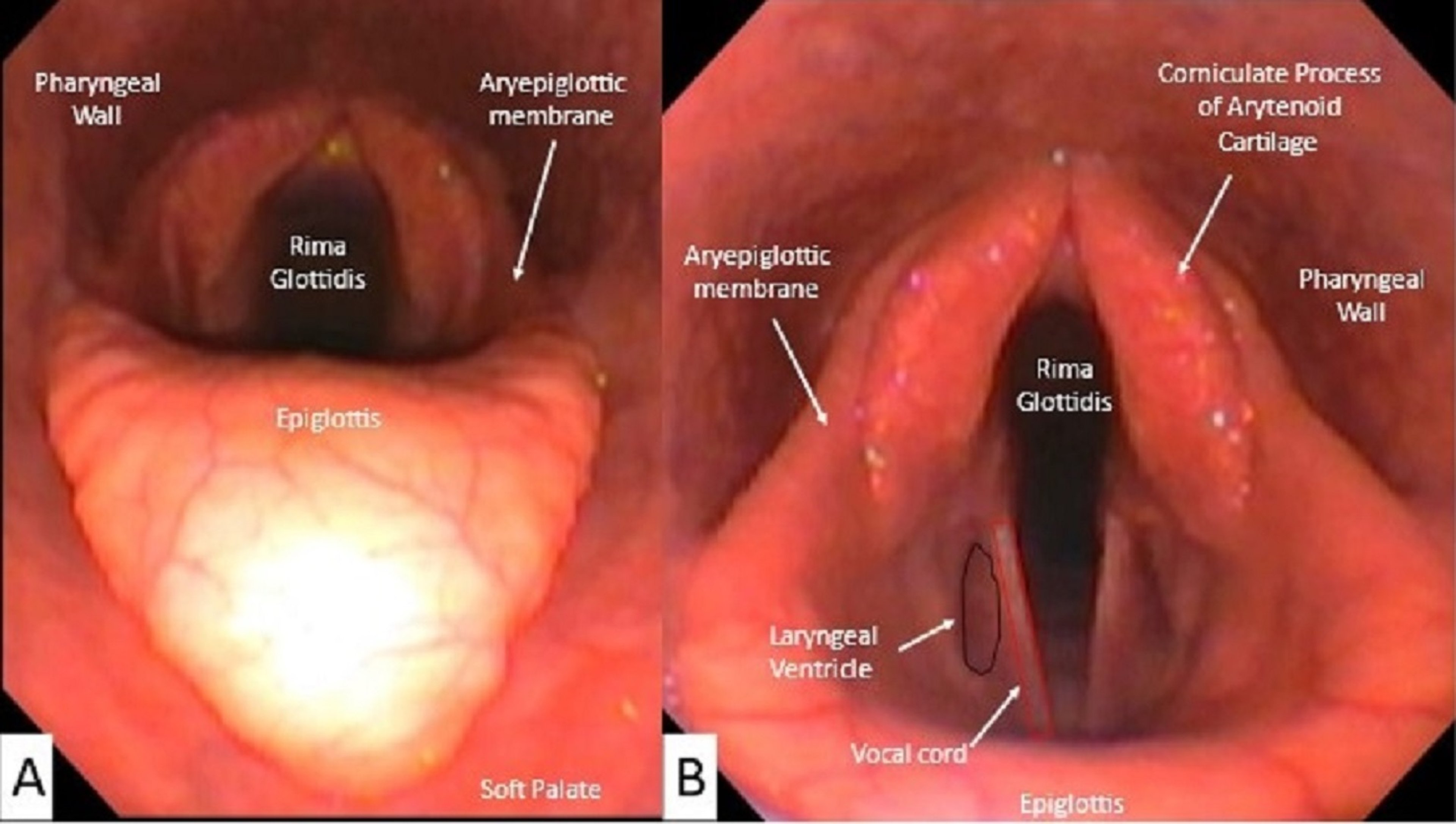
Static endoscopic image of the rostral laryngeal structures viewed during upper airway examination. A. Image obtained with the endoscope placed in the nasopharynx allowing full visualization of the epiglottis B. The endoscope has been advanced toward the trachea
Courtesy of Dr. Lindsey Boone.
Laryngeal hemiplegia results from the progressive loss of the large myelinated fibers in the distal portion of the recurrent laryngeal nerve, which ultimately impairs the abductor function of the cricoarytenoideus dorsalis muscle. The ipsilateral arytenoid cartilage, almost always on the left side, is either partially or completely paralyzed as a result. Axonal dystrophy of the left recurrent nerve occurs more commonly than the right, likely due to its extended length as it courses around the base of the heart before innervational insertion.
Loss of neuromuscular control to the laryngeal abductor muscles results in collapse of the arytenoid cartilage and vocal fold, which reduces the cross-sectional area of the rima glottidis. The resistance to airflow necessitates greater respiratory effort. Because of the pliable nature of the glottidis, this increased effort results in exaggerated subatmospheric pressure within the airway, often resulting in further collapse of the arytenoid cartilage. Upon inspiration during strenuous exercise, the affected side is drawn across the midline (by negative pressure in the airway) until it abuts the abducted normal arytenoid, effectively occluding the airway (dynamic collapse). Horses with paralysis and/or dynamic arytenoid collapse are colloquially labeled as “roarers.” A characteristic inspiratory whistle results from increased resonance within the laryngeal ventricle below the paralyzed arytenoid cartilage. In more severe collapse, a harsher stridor, or roar, is produced due to turbulence from the edges of the collapsed arytenoid cartilage, vocal cord and laryngeal ventricle.
Left laryngeal hemiplegia is likely to be heritable, with a higher prevalence of disease reported in tall Thoroughbred (affecting up to 8% of the population) and draft breeds (affecting up to 35% of heavy draft breeds). Less common causes of neuropathy include direct trauma to the recurrent laryngeal nerve, guttural pouch disorders, accidental perivascular injection of irritating substances, and plant (eg, Cicer arietinum [chickpeas] and Lathyrus spp) or chemical intoxication. Lead toxicity should be suspected in horses with bilateral laryngeal paralysis.
Clinical Findings and Diagnosis of Laryngeal Hemiplegia in Horses
Clinical evaluation
Endoscopic evaluation
Laryngeal ultrasonography
Horses usually present with a history of poor performance and/or exercise intolerance and an inspiratory noise. These findings are typically manifested during intense, high-speed exercise, but completely paralyzed cases can be readily identified on resting endoscopy. Laryngeal palpation may identify a prominent muscular process of the arytenoid cartilage due to muscle atrophy.

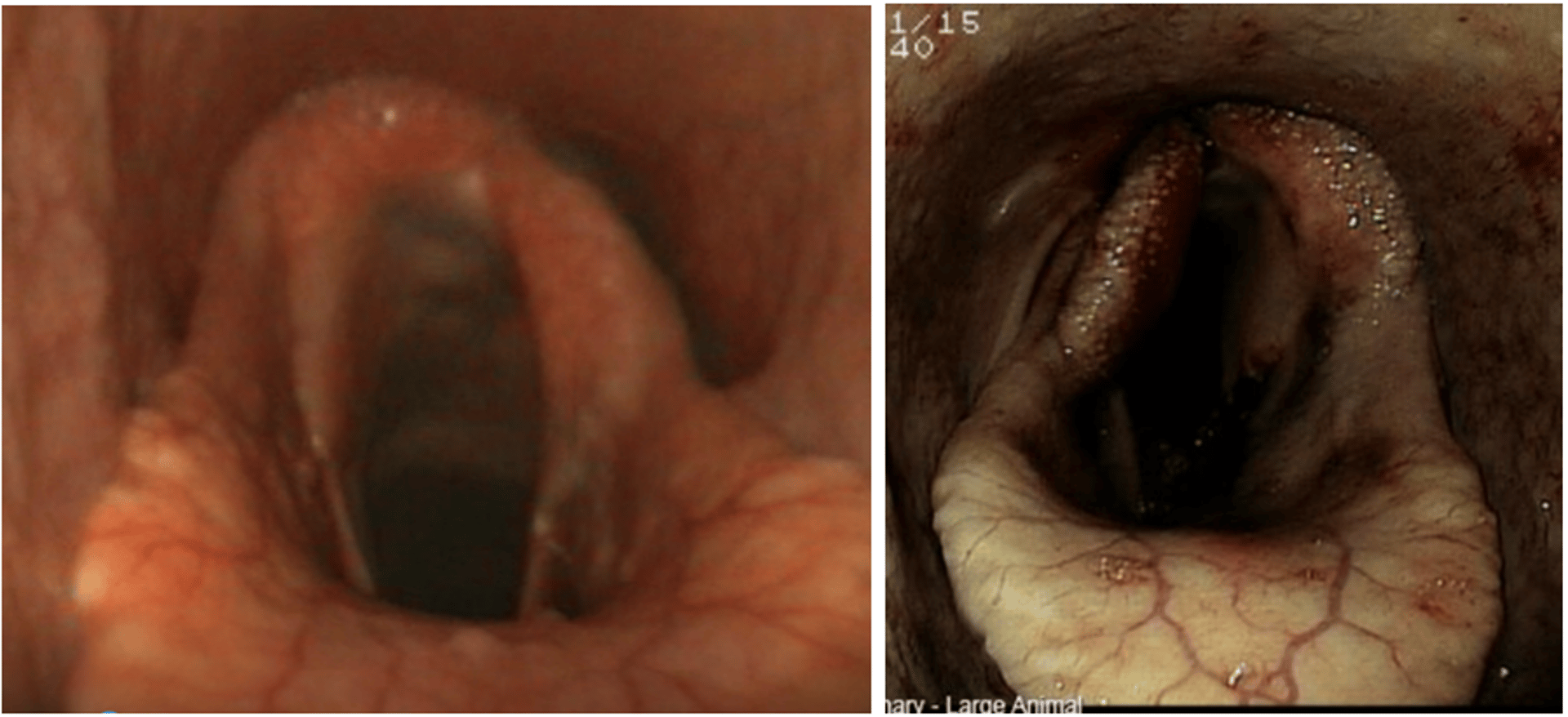
Left: Endoscopic image of horse with a grade IV (complete paralysis) left laryngeal hemiplegia. Note that the right arytenoid is fully abducted while the left arytenoid hangs within the airway. Right: Endoscopic image of horse 24 hours after tie-back procedure. Note that the left arytenoid cartilage is maintained in abduction while the right arytenoid cartilage is imaged in a resting position.
Courtesy of Dr. Lindsey Boone, Auburn University.
Diagnosis is confirmed by endoscopic observation of reduced or absent abduction of the arytenoid cartilage and vocal fold. A grading system, known as the Havemeyer laryngeal grading system, is used for consistency in reporting and understanding recommended treatments (Grade 1 = normal, Grade 4 = completely paralyzed arytenoid). During resting endoscopic examination it is important the horse remain unsedated. Maximal movement of the arytenoid cartilage can be encouraged and observed after inducing swallowing and/or during nasal occlusion. Up to 30% of horses with recurrent laryngeal hemiplegia will have additional dysfunction of the larynx during exercise; therefore, when resting exam findings are equivocal, dynamic (overground) endoscopy is used to aid diagnosis and to guide treatment.
Laryngeal ultrasound can be used to augment findings of a static endoscopic examination. Ultrasonographic abnormalities are observed as a change in echogenicity within the laryngeal abductor muscles (cricoarytenoideus lateralis +/- dorsalis muscle).
Differential diagnoses include other pharyngeal or laryngeal conditions that produce upper airway obstruction and exercise intolerance, such as arytenoid chondritis, nasopharyngeal collapse, and axial deviation of the aryepiglottic folds.
Treatment of Laryngeal Hemiplegia in Horses
Conservative treatment
Surgical treatment
Treatment of recurrent laryngeal hemiplegia should be pursued in light of the presenting complaint (noise and/or exercise intolerance), the patient’s age and intended use (exercise demands), and extent of arytenoid collapse. Many horses can perform with some extent of arytenoid collapse if their intended purpose does not involve intense, high speed exercise; therefore, some horses are diagnosed and monitored, but not treated.
The most common treatment is surgical prosthetic laryngoplasty, which is the treatment of choice in horses with partial or complete paralysis and exercise intolerance. This procedure is also commonly referred to as a “tie-back” procedure because the arytenoid cartilage is tied backward and anchored to the cricoid cartilage, emulating the function of the atrophied and dysfunctional cricoarytenoideus dorsalis muscle. This procedure should result in permanent abduction of the arytenoid cartilage. The abduction that is achieved should be adequate to enhance airflow during exercise; however, it should not be so great that aspiration occurs during swallowing. Prosthetic laryngoplasty is commonly done in racing horses and is the only technique that satisfactorily reduces the impedance to inspiratory flow. Postoperative complications include chronic cough, chronic aspiration of feed, implant failure, and implant infection. Athletic performance will improve after surgery, though the airflow achieved by laryngoplasty is still reduced compared to normal levels.
Ventriculectomy (sacculectomy) is performed alone or in conjunction with prosthetic laryngoplasty and refers to surgical removal of the mucosal lining of the laryngeal ventricle. This procedure is performed to decrease the noise present during inspiration with recurrent laryngeal neuropathy.
Ventriculocordectomy refers to removal of the leading edge of the vocal fold and the mucosal lining of the laryngeal ventricle. Ventriculectomy or ventriculocordectomy can be performed either via a laryngotomy or transendoscopically in the standing, sedated horse using a surgical diode laser. These procedures are considered for horses that make a noise, but are not exercise intolerant.
Laryngeal reinnervation is only pursued in young horses with partial paralysis and requires surgical dissection, transfer, and implantation of a neuromuscular pedicle graft into the cricoarytenoideus muscle.
Partial arytenoidectomy refers to removal of the muscular +/- the corniculate process of the arytenoid cartilage typically only pursued for recurrent laryngeal neuropathy if complications or failure of the prosthetic laryngoplasty have occurred.
Key Points
Laryngeal hemiplegia is the result of recurrent laryngeal neuropathy, causing partial or complete loss of arytenoid abduction.
Laryngeal hemiplegia almost always occurs on the left side of the larynx.
Clinical signs of laryngeal hemiplegia are inspiratory noise (whistle or roar) and/or poor performance/exercise intolerance.
Surgery is aimed at reducing noise and stabilizing the arytenoid in a permanent, partially abducted position.
For More Information
Workshop Report. Consensus statements on equine recurrent laryngeal neuropathy: conclusions of the Havemeyer workshop. Equine Veterinary Education (2004) 16 (6) 333–336.
Davenport-Goodall C & Parente E. Disorders of the larynx. Veterinary Clinics: Equine Practice (2003)19 (1): 169–187.
Woodie J.B. Evaluation of the Upper Respiratory Tract at Rest and During Exercise. In Depth: Respiratory. AAEP Proceedings. 2011. 57: 1–4.
Also see pet health content regarding disorders of the larynx in horses.





