

Owners can use well-ventilated plastic enclosures with moistened paper towels for the transport of most amphibian species to veterinary clinics. Owners should pay special attention to environmental temperatures during transport to prevent heat or cold stress. Veterinarians must consider that exposure to outdoor temperatures during transport may greatly affect an amphibian’s mentation. On arrival at the clinic, amphibians should be kept within their preferred optimal temperature zone (POTZ) because rooms typically used for housing reptiles are unsuitably warm for most amphibian species.

Courtesy of Dr. Taylor Yaw.
A veterinarian should start an examination with a thorough history, including a description of the patient’s diet and appetite, environmental conditions (humidity, temperature gradient, light cycle, light type and positioning), reproductive status, recent animal introduction or losses, medication and disinfection protocol, and water quality measurements. A review of food and water quality records is useful to identify noteworthy trends. Special attention must be given to vitamin and mineral supplementation type and application. Photographs of the enclosure can be valuable to assess husbandry setup and practices. A water sample from the animal’s enclosure should be analyzed for ammonia, nitrate, nitrite, pH, hardness, alkalinity, chlorine, and potentially heavy metals using a simple test kit readily available from most pet stores. Veterinarians should consider confirming test results outside normal parameters using commercial water testing facilities. Owners must take and record air and water temperatures at the time of water collection.
Before handling, the patient’s body condition, agility, posture, and behavior should be observed. Respiratory effort, including gular movement and pulmonary respiration, should be observed. Neurologic impairment may be suspected if an amphibian is unable to maintain equilibrium or exhibits an abnormal swimming pattern. Fecal or egg production should be visually assessed before handling.
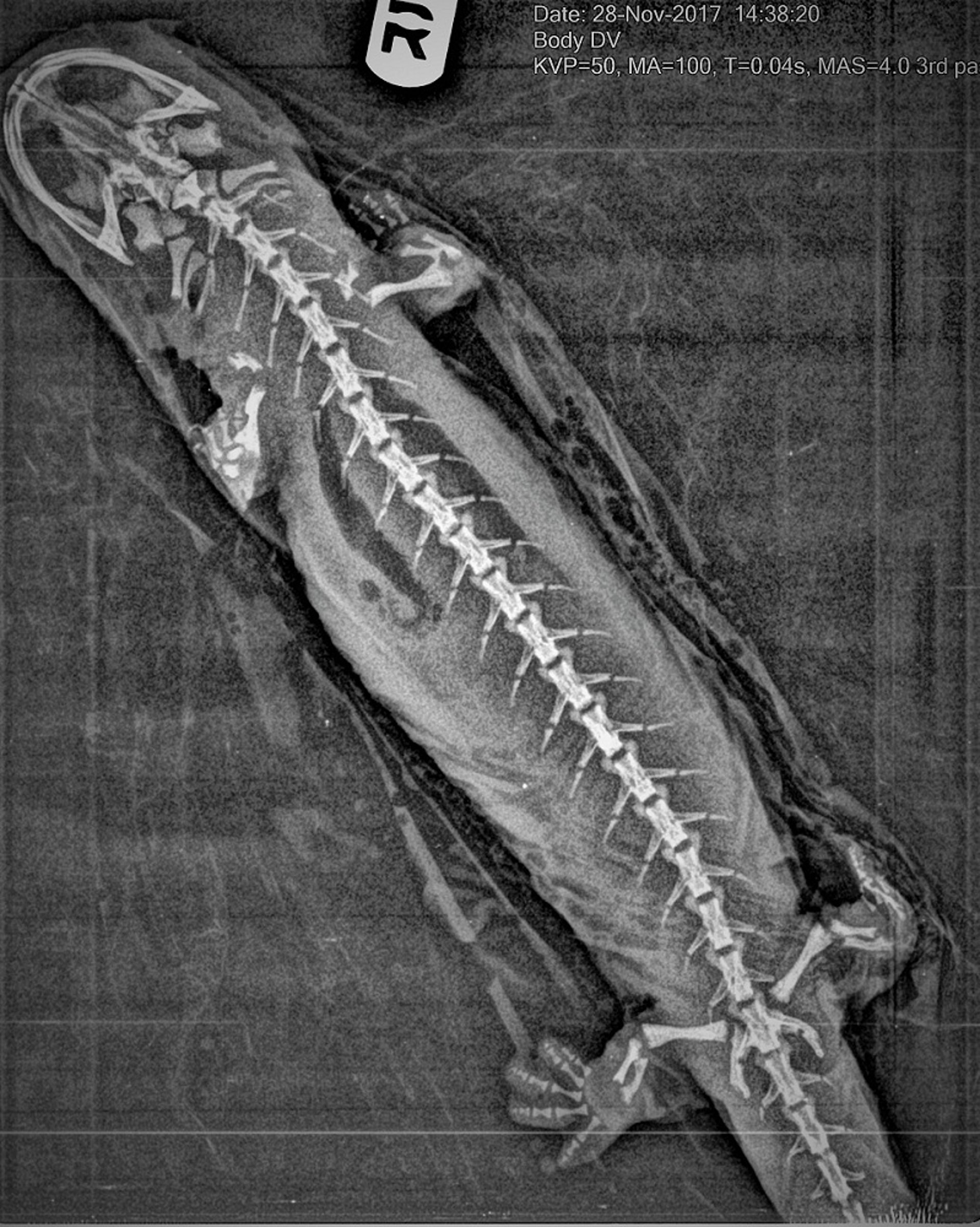
Before handling the patient, all possible routes of escape from the examination room, such as ventilation ducts and sink drains, should be blocked. The temperature of the examination room should be 21°–24°C or within the animal’s POTZ, when known. Restraint should be done wearing moistened, powder-free vinyl gloves (not latex). Gloves should be changed between patients to avoid infectious disease transmission, and handling should be kept to a minimum to avoid heat stress and death due to heat conduction transfer from the palm of the hand. Atraumatic dip nets, plastic bags with enclosure water, or damp towels can be used to restrain slippery patients. Amphibians can be placed in a moistened zip-top bag for short periods to obtain radiographs or perform ultrasonography. Caution must be exercised to ensure that all equipment used in direct contact with amphibians is free of toxic residue from disinfectants.

Courtesy of Dr. Taylor Yaw.
When handled, most healthy amphibians attempt to escape, withdrawing limbs that are grasped. Many amphibians bite.
A cool, bright light and magnification are needed when performing a physical examination. Light sources should be used to transilluminate the coelomic cavity and other body areas for further assessment. Slit lamps not only aid in evaluation of ocular structures but can also be used to view external lesions.
The patient's mouth can be opened using the edge of an index card, a plastic card, thin guitar pick, or a rubber spatula. The color of the mucous membranes should be evaluated and any lesions recorded. Touch preparations or skin scrapings of epidermal lesions should be collected for cytologic evaluation. Heart rate can often be determined by watching the skin overlying the xiphoid or using a Doppler ultrasonic probe. Because pulmonic respiration (if present) depends on positive-pressure ventilation from buccal pumping, respiratory rate should be assessed by watching the rapid movements of the intermandibular space (ie, gular respiration). The nares should be free of obstruction from mucus and bubbles, which may indicate respiratory disease. Eggs or larvae of many respiratory parasites (eg, Rhabdias spp) may sometimes be detected in oropharyngeal mucus.
Ocular lesions may include conjunctival, corneal, iridal, and lenticular changes. Corneal diseases, including nonspecific keratitis and lipid keratosis, are common. Coelomic palpation may detect retained egg masses, bladder stones, foreign bodies, or neoplasms. Hydrocoelom and subcutaneous edema (anasarca and ascites) are common. Fluid collected via ultrasound-guided aspiration should be assessed by biochemical analysis and cytologic evaluation. Culturing for bacteria and fungi is recommended. Transcoelomic illumination with a bright light source can greatly aid in assessment of coelomic distension.


Courtesy of Dr. Taylor Yaw.
Blood collected from the ventral abdominal vein, lingual vein, femoral vein, coccygeal vein or via cardiac puncture and placed into lithium heparin blood collection tubes can be used for hematologic evaluation. A bright light source can be used to transilluminate targeted veins. Pretreatment of the syringe with lithium heparin should be avoided due to potential dilutional affects. A volume equal to 1% of the body weight of a healthy amphibian and 0.5% of the body weight of a sick amphibian may be taken. Normal values have not been established for most species of amphibians. However, cell morphology and reactive changes can aid in clinical diagnosis. Urine may be collected for analysis from those anurans that urinate when first restrained. Fecal samples uncontaminated by environmental organisms may be collected from species such as dart frogs by feeding the animal just before placing it on a clean, moist paper towel. Direct and float examinations are useful to identify protozoa and metazoa.


Courtesy of Dr. Taylor Yaw.
Treatments can be administered orally, topically, by immersion, or by injection. Oral administration of medications requires firm restraint and opening the patient's mouth. Microliter syringes and pipettes should be used for accurate medication. Many drugs can be administered topically due to the permeable nature of amphibian skin. Some drugs, such as enrofloxacin, may be irritating, and alternative routes of administration may be preferred. Treatments can also be delivered topically by placing the amphibian in a medicated bath. Bubble wrap or other nonabrasive material placed strategically over the amphibian may be needed to keep it in contact with the solution.
When choosing treatment routes, veterinarians should consider which treatment option would result in the smallest amount of stress with maximal drug absorption. Amphibians with primary integument or gastrointestinal disease may not readily absorb medications by topical or oral routes, respectively. Injections are typically administered IM, intracoelomically, into the lymph sacs, or IV.


Courtesy of the National Aquarium.


Courtesy of Dr. Brent Whitaker, National Aquarium.
Anesthesia of Amphibians
Due to amphibians' small size and delicate integument, sedation or light anesthesia can enhance the quality and safety of physical examination and aid in adequate diagnostic sample collection. Use of several anesthetic agents, mostly delivered via immersion, has been reported in amphibian species. Responses to these sedative agents are variable across species, affected by environmental parameters and the patient’s health. Tricaine methanesulfonate (MS-222), ketamine hydrochloride, propofol, alfaxalone, isoflurane, and sevoflurane may be used. Immersion anesthetics should be prepared in water of a neutral pH and free of other contaminants. Larger amphibians can be intubated and maintained on anesthetic gas after induction. Injections into the rear limbs are avoided because of the presence of a renal-portal system.
Tricaine methanesulfonate is a fine, white crystal highly soluble in water. It can be prepared and stored as a 10 g/L stock solution and diluted just before use. Tricaine methanesulfonate produces an acidic solution that must be buffered (eg, with sodium bicarbonate, sodium hydroxide, or sodium hydrogen phosphate). Administration is by bath, because most amphibians absorb tricaine methanesulfonate through the skin. Small, plastic bags or plastic containers with lids can be used for induction. The dosage used for many large amphibians is 1–3 g/L for anesthetic induction, whereas in tadpoles a much lower anesthetic induction dose of 0.5 g/L should be used. For short procedures, the amphibian should be immediately removed and rinsed with fresh water. For longer procedures, the amphibian may be placed into a maintenance solution of 0.1–0.4 g/L because depth of anesthesia is time and concentration-dependent with immersion treatment. Aeration must be provided in the anesthetic solution to avoid hypoxia, and oxygen saturation in the water can be maintained close to 100% (determined by dissolved oxygen probe).
Isoflurane gas can also be bubbled into an anesthetic bath, placed in a sealed container, or placed in sterile lube for topical application. However, this can result in dangerously deep planes of anesthesia and exposure of anesthetic gas to personnel. Furthermore, time to induction of anesthesia can be markedly prolonged with inhalant anesthetics, especially in species that can convert to anaerobic metabolism.
Ketamine hydrochloride injected percutaneously or into the dorsal lymph sac at a dosage of 75–125 mg/kg can be used; however, a surgical plane of anesthesia can be difficult to maintain, and recoveries are long, with muscular contraction causing a sawhorse stance. Propofol has been documented as an anesthetic administered topically or via intracoelomic or IV injections (9–30 mg/kg); however, it results in inconsistent anesthetic induction times, depth of anesthesia, and recovery times.
Alfaxalone, a neuroactive, synthetic steroid, has been used as a sedative agent in a wide range of species. Dose ranges seems to depend on species and temperature. In general, much higher doses of alfaxalone are needed (20–30 mg/kg) for anuran species, whereas caudatan species need much less (< 10 mg/kg) for similar levels of sedation. Alfaxalone seems to have negligible pain modulation, so additional analgesic administration is suggested.
Amphibians demonstrate a dose-dependent analgesic response to opioids and α2-receptor agonists (eg, dexmedetomidine). Reported analgesic doses range widely (from 0.15–0.60 mg/kg, SC1 or IM, to 40–120 mg/kg, SC2). However, doses of 10 mg/kg did not produce sedation in frogs, with animals retaining corneal, righting, and hind limb withdrawal reflexes.3
A baseline heart rate should be established before initiating anesthesia. It can be obtained from some amphibian species before restraint with placement of ultrasonic gel on the bottom of a thin, plastic container and using a Doppler ultrasonic probe. Electroencephalogram needles can be used in amphibians to obtain ECGs. Because amphibians can breathe through the skin, observing gular movement is an inaccurate predictor of perfusion and oxygenation.
References
Whiteside DP. Don't Let it Croak: Clinical Approach to Amphibian Emergencies. 67th Convention of the Canadian Veterinary Medical Association, 2015.
Wright KM. Chapter 90: Amphibian formulary. In: Divers S, Stahl S, eds. Mader's Reptile and Amphibian Medicine and Surgery. 3rd ed. Elsevier, 2017;1140-1146.
Brenner G, Klopp A, Deason L, et al. Analgesic potency of alpha adrenergic agents after systemic administration in amphibians. J Pharmacol Exp Ther 1994; 270:540–545.
Euthanasia of Amphibians
Verification of death can be difficult because the amphibian heart continues to beat after death. An ECG, Doppler ultrasonic probe, or conventional ultrasonography can be used to determine death; however, physical intervention (pithing, rapid freezing if < 4 g, or decapitation) under general anesthesia should be considered. Overdoses of injectable anesthetic agents (ketamine, tiletamine-zolazepam, propofol, or alfaxalone) can be used to induce anesthesia before a physical intervention.
If available, immersion in buffered tricaine methanesulfonate (5–10 g/L) or benzocaine hydrochloride (≥ 250 mg/L) can be used to induce anesthesia.
Although inhalant anesthetics can be used to induce anesthesia, many amphibians are capable of breath holding and blood shunting, which prolong induction of anesthesia.
Hypothermia is an unacceptable method of euthanasia unless the animal is sufficiently small (< 4 g) to permit immediate and irreversible death in liquid nitrogen. Intracardiac administration of euthanasia agents should not be conducted in amphibians unless they are unresponsive to stimuli. Freezing or maceration of eggs is likely appropriate, resulting in instantaneous death. Larval stages should be euthanized as per adults.
For More Information
Divers S, Stahl S, eds. Mader's Reptile and Amphibian Medicine and Surgery. 3rd ed. Elsevier, 2017.
AVMA Guidelines for the Euthanasia of Animals: 2020 Edition.
Also see pet health content regarding amphibians.





