



Swine dysentery is a mucohemorrhagic diarrheal disease of pigs that is limited to the large intestine. Swine dysentery is most often observed in growing-finishing pigs and is associated with decreased growth performance and variable mortality rates.
Etiology and Pathogenesis of Swine Dysentery
Swine dysentery has historically been associated with only Brachyspira hyodysenteriae infection. However, two other species of Brachyspira have been confirmed as etiological agents of swine dysentery: B hampsoniiandB suanatina. All three of these spirochetes consistently produce strong beta hemolysis when cultivated on blood agar under anaerobic incubation conditions.
Transmission is fecal-oral, and sources of infection include feces from infected pigs, contaminated lagoon water, and contaminated transport vehicles. Once ingested, Brachyspira proliferate in the large intestine and cause superficial mucosal degeneration and inflammation, mucosal epithelial hypersecretion of mucus, and mucosal surface multifocal hemorrhage. Decreased ability of the mucosa to reabsorb endogenous secretions results in diarrhea.
Clinical Findings of Swine Dysentery
The first clinical signs of swine dysentery are often anorexia and passage of soft feces. The course of the disease is variable; typically, however, diarrhea increases in severity and quickly becomes mucohemorrhagic, with copious mucus and frank blood. Prolonged disease leads to dehydration, hollow flanks, and marked weight loss. Disease progresses through groups of pigs, and morbidity rates can exceed 50%, with 30% or more mortality if left untreated.
Lesions of Swine Dysentery
Lesions are confined to the cecum, spiral colon, descending colon, and rectum. Moderate mesocolonic edema may be observed, and mucosal lesions are often present at the apex of the spiral colon (see ). The affected mucosa is variably swollen and covered with a layer of transparent to slightly opaque mucus, often with suspended flecks of blood. As disease progresses, a mixture of blood, fibrin, and necrotic debris accumulates in the colonic lumen.

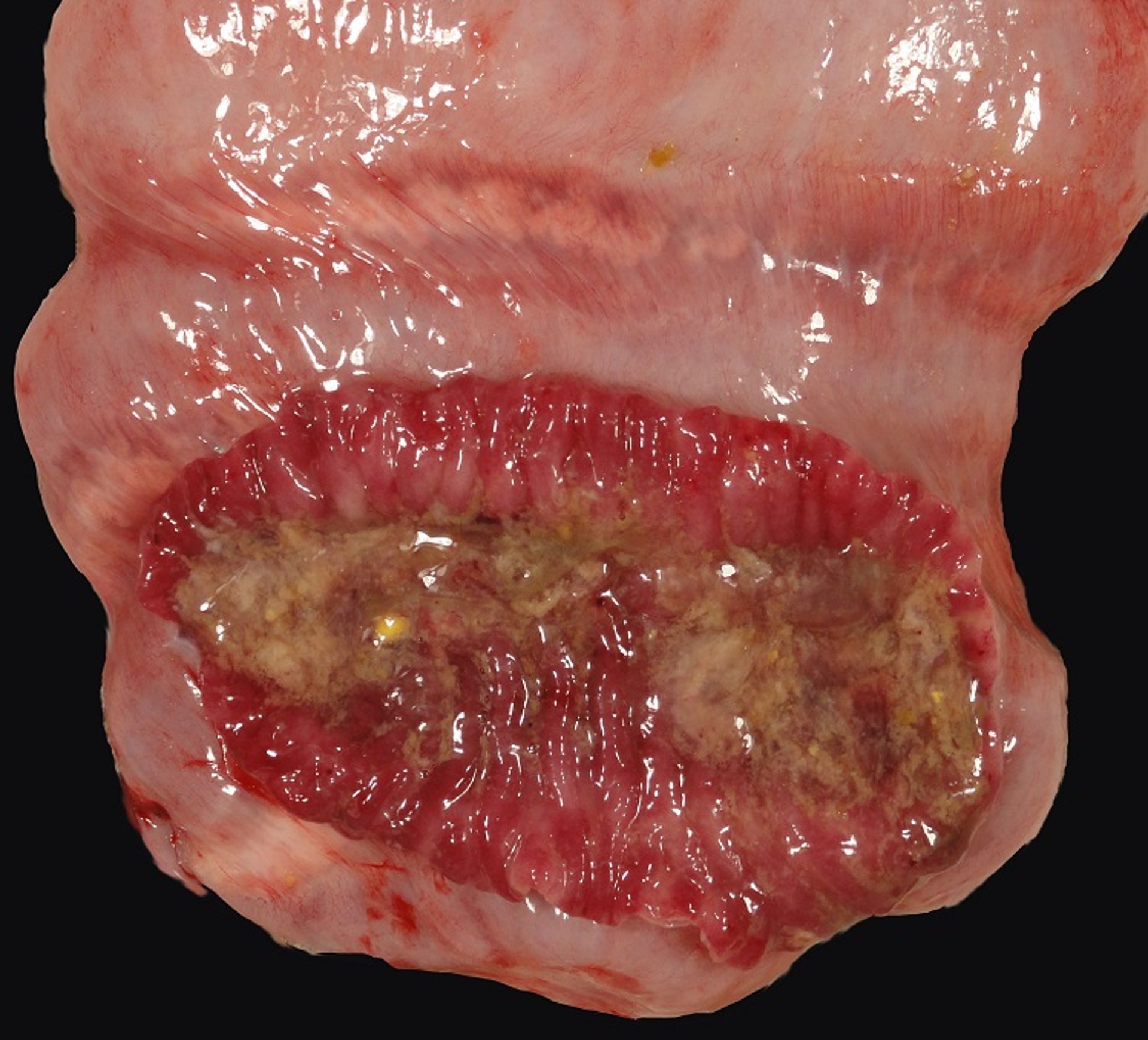
Gross lesions in the spiral colon typical of acute swine dysentery in a pig. Note the mucosal congestion and hemorrhage with abundant luminal mucus in the opened loop at the apex of the spiral colon. Mild to moderate mesocolonic edema between loops is also present in this image and is common in acute disease.
Courtesy of Dr. Eric R. Burrough.
Microscopically, there is a moderate typhlocolitis that progresses from superficial neutrophilic inflammation in acute cases to lymphoplasmacytic with marked goblet cell hyperplasia with chronicity.
Diagnosis of Swine Dysentery
Selective anaerobic culture with or without PCR assays
Histological evaluation
Clinical signs and postmortem examination findings are usually sufficient for a presumptive diagnosis of swine dysentery.
Confirmation of diagnosis is based on demonstration of typical histological lesions in the large intestine and isolation of strongly beta-hemolytic Brachyspira by anaerobic culture. (See of B hyodysenteriae.)


Note the characteristic morphology of Brachyspira hyodysenteriae: loose, slender coils. Other agents of swine dysentery have similar morphology and can often be visualized in stained fecal smears from clinically affected pigs.
Courtesy of Joann Kinyon, Iowa State University Veterinary Diagnostic Laboratory.
PCR assays are available for many agents of swine dysentery; however, bacterial culture is preferred for confirmation of hemolytic phenotype because atypical weakly hemolytic isolates of B hyodysenteriae have been reported.
Differential diagnoses often include intestinal spirochetosis, proliferative enteropathy, intestinal salmonellosis, and heavy whipworm infections. Polymicrobial infections are common.
Treatment and Control of Swine Dysentery
Administration of antimicrobials based on results of minimum inhibitory concentration testing
Biosecurity and rodent control
Antimicrobials are an effective treatment for swine dysentery if started early, and water medication may be preferred. Increasing resistance to antimicrobials has been reported in several countries; thus, minimum inhibitory concentration testing is recommended before starting antimicrobial treatment. Pleuromutilins, lincomycin, and tylosin are commonly used.
Swine dysentery can be eradicated from infected premises without total depopulation by implementing a persistent and carefully planned program that includes treatment of carrier pigs with antimicrobials and thorough cleaning and disinfection of vacated facilities.
Rodents and waterfowl are important reservoirs for Brachyspira spp, and any eradication attempt must include eliminating or decreasing exposure to these reservoirs on the farm. Expression of swine dysentery is strongly influenced by diet and can be decreased through alteration of dietary fiber—ie, feeds containing more soluble fiber, such as sugar beet pulp, can be fed in place of feed components high in insoluble fiber, such as distillers dried grains with solubles (1).
Key Points
Swine dysentery is characterized by mucohemorrhagic diarrhea of variable severity.
Dysentery-associated Brachyspira spp all produce strong beta hemolysis when cultivated on blood agar.
Expression of swine dysentery is strongly influenced by diet.
For More Information
Burrough ER. Swine dysentery: etiopathogenesis and diagnosis of a reemerging disease. Vet Pathol. 2017;54(1):22-31.
Hampson DJ, Burrough ER, Costa MO. Brachyspira spp. In: Zimmerman JJ, Burrough ER, Karriker LA, Schwartz KJ, Zhang J, eds. Diseases of Swine. 12th ed. John Wiley and Sons, Inc; 2026:891-911.
References
Helm ET, Gabler NK, Burrough ER. Highly fermentable fiber alters fecal microbiota and mitigates swine dysentery induced by Brachyspira hyodysenteriae. Animals. 2021;11(2):396. doi:10.3390/ani11020396





